3 Chapter 3: Ageism
Tracy Everitt; Brittany Yantha; Megan Davies; and Laurie Wadsworth
Chapter 3 Learning Objectives
At the conclusion of this chapter, students will be able to:
Learning Objectives
- Understand the concept of ageism and recognize how this form of oppression is perpetuated through our daily actions and through the media.
- Explain how ageism contributes to poor health in older adults.
- Describe how COVID-19 and ageism contributed to poor health in older adults.
- Identify strategies to overcome ageism.
- Describe how other forms of discrimination and poverty impact health status for aging adults.
Introduction
Stereotypes about older adults lead many to assume that all older adults have poor health and experience mental decline. These stereotypes are reflected in everyday conversations, the media, and even greeting cards. Ageism is prejudice and discrimination directed towards people solely based on age, and societal attitudes about aging are examples of ageism.
Ageist attitudes suggest that older people are less in command of their mental faculties and are feeble and ill. Older people are viewed more negatively than younger people on various traits, particularly general competence and attractiveness. Stereotypes such as these can lead to a self-fulfilling prophecy in which beliefs about one’s ability result in actions that make it come true. Ageism can combine with other factors and further compromise health. For example, the negative stereotypes associated with ageism around the capacity of older adults during the COVID-19 pandemic contributed to increased rates of disease, social isolation, and loneliness (Brooke & Jackson, 2020).
3.1 Ageism
Societal stereotyping towards older adults and the process of aging can lead people to assume, often unconsciously, that aging automatically brings poor physical health and mental decline, when in fact, many older adults may experience good health with preserved cognitive function. The conscious and unconscious negative attitudes people have toward aging are examples of ageism. Ageism is the process of systematic stereotyping or discrimination against people based on their age. This stereotyping and discrimination draws similarities to racism and sexism. These oppression systems all lead to poorer health outcomes, social isolation, increased morbidity and mortality, and a lower economic status. The term ageism was first used in 1969 by Dr. Robert Butler, and according to Nelson (2016), ageism remains one of the most institutionalized forms of prejudice today.
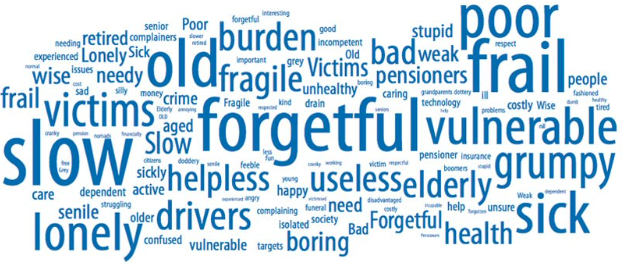 Figure 3.1.1 Words used to describe the elderly are often negative and biased.
Figure 3.1.1 Words used to describe the elderly are often negative and biased.
Source: https://www.humanrights.gov.au/our-work/chapter-4-role-and-influence-media.
The word cloud in Figure 3.1.1 is from research conducted by the Australian Human Rights Commission. They polled people on the following question: “Thinking about everything you see and hear in the media (including on TV, online, on the radio and in newspapers and magazines), how do the media portray older people?“ Their responses are listed here, with the larger words being listed more often. Ageism can also affect self-identity or feelings of self-efficacy, as growing older is often associated with growing useless.
Ageism has direct impacts on health. Memory and cognitive skills declined in older adults who believed negative stereotypes about aging people (Nelson, 2016). In contrast, older individuals in cultures such as China that held more positive views on aging demonstrated fewer cognitive deficits (Nelson, 2016).
Being the target of stereotypes can adversely affect individuals‘ performance on tasks because they worry they will confirm the cultural stereotypes. This is known as stereotype threat, and it was initially used to explain race and gender differences in academic achievement (Gatz et al., 2016). Research on stereotype threat has demonstrated that older adults who internalize the aging stereotypes will exhibit worse memory performance, worse physical performance, and reduced self-efficacy (Levy, 2009).
Ageism, reinforced through the media by overwhelmingly negative portrayals, is harmful and contributes to the general public’s perceptions of aging. There is a lack of representation of older adults in acting and modelling positions which controls what people see in media (Levy, 2009). The ideals of beauty are tied to youthfulness and reversing the process of aging. Older adults are often portrayed as helpless victims, and those who defy these negative stereotypes are perceived as bizarre or comical. Overall, aging is underrepresented or ignored by the mass media or portrayed as having less value. These representations could create lasting impressions of negativity and shame among older adults (Levy, 2009).
Not only do pervasive ageist attitudes and stereotypes contribute to negative health outcomes, but ageism among healthcare professionals can also result in discriminatory practices that place older people at risk. Studies have found widespread negative attitudes toward older people and old age among physicians, medical students, and nurses (Burnes et al., 2019). Such ageist attitudes can impact health service delivery, as assumptions regarding functional and cognitive decline lead to more limited provision of medical information, withholding of certain treatment options, and exclusion from clinical trials (Burnes et al., 2019). Ageist attitudes, such as assuming that depressive symptoms are normal among older adults have also been found among mental health practitioners and trainees , which may restrict access to treatments or under-treatment of disease states (Burnes et al., 2019). Therefore, age stereotyping and prejudice among health providers can affect the quality and quantity of care older people receive, leading to negative health outcomes.
Those who believe in negative stereotypes are less likely to engage in preventative health behaviours, less likely to recover from illnesses, and more likely to feel stress and anxiety, which can adversely affect immune functioning and cardiovascular health (Nelson, 2016). Individuals who attribute their health problems to their age also have a higher death rate. Similarly, doctors who believe that illnesses are just natural consequences of aging are less likely to have older adults participate in clinical trials or receive life-sustaining treatment. In contrast, those older adults with positive and optimistic views of aging are less likely to have physical or mental health problems and are more likely to live longer. Removing societal stereotypes about aging and helping older adults reject stereotypical notions of aging is another way to promote health and extend life expectancy. However, an even better way is for societies to promote the full inclusion of us all at every age.
3.2 Ageism and COVID-19
The COVID-19 pandemic changed how older adults are treated and perceived. The distinction between young and old and the language surrounding this issue is stressed in current public discourse, which reinforces the already age-divided societies (Ayalon et al., 2021). Chronological age, chronic illness, and comorbidities make individuals more vulnerable to COVID-19. In emergencies, older adults with cognitive or physical impairments face even greater risks of losing autonomy and having their human rights violated. Physical distancing practices and the increasing reliance on digital technology may be a challenge for older adults with limited access or ability to use technology, contributing to depression and loneliness (Ayalon et al., 2021). These practices were challenging for some older adults as these practices prevented seniors from accessing goods and services and obtaining the social support they needed during the outbreak.
Ageism evident through phrases such as #BoomerRemover has been trending on social media platforms. This specific phrase is slang for the COVID-19 outbreak that refers to the higher chances of boomers dying or in other words, being removed. It was often accompanied by ageist disparaging and devaluing memes, media coverage, online discussions, and commentary about the potential for rationing care, with older people being disadvantaged and positioned as more expendable than younger people (Brooke & Jackson, 2020). These ageist discourses and the subtext of negativity and devaluing of older people can and will contribute to feelings of worthlessness in older people, a sense of being burdensome and having no value. When considered in relation to social restrictions caused by the COVID-19 pandemic, these factors make older people particularly vulnerable to a range of negative health and social outcomes, particularly social isolation and loneliness. The impact of social isolation and loneliness on older people’s physical and mental health has been recognized for over two decades (Brooke & Jackson, 2020).
3.3 Overcoming Ageism
There are numerous key strategies healthcare professionals can use to mitigate ageism. These include adopting an individualized, person-centered treatment approach, defining non-ageist practices and attitudes, and acknowledging the need to eliminate ageism in practice. Interventions, including education, intergenerational contact, and combined programs (including those that are small-scale and low-cost), effectively reduce ageism through a change in attitudes and knowledge, leading to improved health and well-being (Burnes et al., 2019). It is important that all people gain an appreciation and positive attitude towards aging since we are always aging and this experience is not unique to any one group of individuals. Advocating for the health and wellness of older adults is crucial for maintaining a healthy social environment. Advocacy raises consciousness and helps to increase awareness, community support, and opportunities for older adults. This can help support their quality of life and well-being through aging. The Global Report on Agism found through the World Health Organization outlines a framework for action to reduce agism including specific recommendations for different actors (e.g. government, UN agencies, civil society organizations, private sector). It brings together the best quality and available evidence on the nature and magnitude of agism. An example of how agism can be reduced is to older adults for their multiple roles in society – as caregivers, volunteers, and community leaders (WHO, 2021).
3.4 Minority Status
In Canada, a person is considered a visible minority group if they are non-white in colour. In addition to ageism, racism is another concern for minority populations as they age. Racism towards members of visible minorities throughout their lifetime results in many older minorities having more chronic health conditions, fewer resources, and significant health disparities when compared to older white people. While white older adults do experience a lack of access exacerbated by ageism, those who are considered a minority experience a further lack of access as compared to white older adults. Racism towards older adults from diverse backgrounds has resulted in them having limited access to community resources such as grocery stores, housing, health care providers, and transportation (Gatz et al., 2016).
No data is available regarding the number of Canadians aged 65 and older who identify as members of the LGTBQ community. Many LGBTQ people have grown older convinced that it is better to keep their sexual orientation or gender identity a secret to ensure their well-being (Government of Canada, n.d.). While some LGBTQ seniors may continue to experience discrimination due to their sexual orientation or gender identity, they may also experience other types of discrimination, such as ageism, sexism, or racism. These factors all contribute to the risk of social isolation and invisibility in LGBTQ seniors, making it challenging to collect data on this group and determine their needs. This is the same with other minority groups in Canada. The intersections of these forms of oppression can create further distress in older adults.
Being an older adult with a minority gender identity can impact health status. The Government of Canada has provided a supplemental toolkit regarding the social isolation of seniors with a focus on LGBTQ seniors in Canada. For more information, see the following link: (https://www.ourcommons.ca/Content/Committee/421/HESA/Reports/RP10574595/hesarp28/hesarp28-e.pdf).
3.5 Poverty Rates
The Canadian income survey released in 2019 reported the median incomes and Canada’s official poverty rate, which is assessed against the Market Basket Measure. The Market Basket Measure refers to the measure of low income based on the cost of a specific basket of goods and services representing a modest, basic standard of living developed by Employment and Social Development Canada (ESDC). The threshold represents the costs of specified qualities and quantities of food, clothing, footwear, transportation, shelter, and other expenses for a reference family of two adults and two children (Statistics Canada, 2017). This measurement estimates the share of the population that does not have sufficient income to afford the cost of a basket of essential goods and services (Government of Nova Scotia, 2021). As seen from Image 3.3.1, poverty rates among older Canadians have been trending down; however, data on the impacts of COVID-19 still must be collected. The pandemic created new challenges specific to older adults. It was harder to leave the house, and access necessary care, leading to social isolation and decreased mental health.
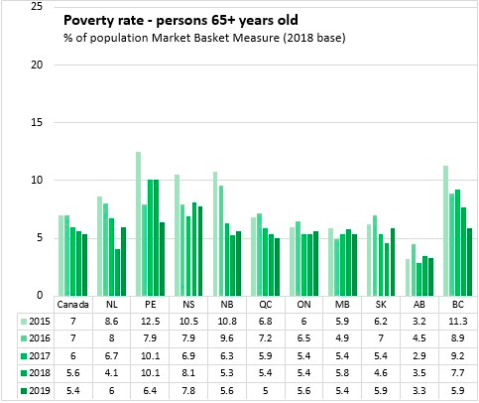
Figure 3.3.1: Although poverty rates for those aged 65 and older are lower, Nova Scotia reports the highest poverty rate in the country for this age cohort (7.8%). National poverty among older Canadians was 5.4% with a low of 3.3% in Alberta
Though data is lacking in Canada on poverty levels among older adults of racial or social minorities, there is information in this regard from the U.S. According to Quinn and Cahill (2016), the poverty rate for older adults in the U.S. varies based on gender, marital status, race, and age. Women aged 65 or older were 70% more likely to be poor than men, and older women aged 80 and above have higher poverty levels than those younger. Married couples are less likely to be poor than nonmarried people, and poverty is more prevalent among older racial minorities. In 2012 the poverty rates for white older men (5.6%) and white older women (9.6%) were lower than for black older men (14%), black older women (21%), Hispanic older men (19%), and Hispanic older women (22%).
This chapter is adapted from ‘Always Developing’ by Anne Baird: https://ecampusontario.pressbooks.pub/alwaysdeveloping/
Creative Commons Attribution: BY NC SA
References
Ayalon, L., Chasteen, A., Diehl, M., Levy, B., Neupert, S., Rothermund, K., Tesch-Romer, C., Wahl, H. (February, 2021). Aging in times of the COVID-19 pandemic: avoiding ageism and fostering intergenerational solidarity. The Journals of Gerontology; Series B, 72:2, e49-e52 https://doi.org/10.1093/geronb/gbaa051
Brooke, J. and Jackson, D. (2020), Older people and COVID-19: Isolation, risk and ageism. Journal of Clinical Nursing, 29: 2044-2046. https://doi.org/10.1111/jocn.15274
Burnes, D., Sheppard, C., Henderson Jr, C. R., Wassel, M., Cope, R., Barber, C., & Pillemer, K. (2019). Interventions to reduce ageism against older adults: A systematic review and meta-analysis. American Journal of Public Health, 109(8), e1-e9.
Cousins, S. O. B. (2005). Overcoming Ageism in Active Living. Retrieved from https://www.activeagingcanada.ca/participants/projects/ageism.htm
Gatz, M., Smyer, M. A., & DiGilio, D. A. (2016). Psychology’s contribution to the well-being of older Americans. American Psychologist, 71(4), 257-267.
Government of Canada (2022, April 20). About the new horizons for seniors program. Retrieved October 5, 2022, https://www.canada.ca/en/employment-social-development/programs/new-horizons-seniors.html
Government of Nova Scotia. (2021, March 23). Nova Scotia Department of Finance – Statistics. https://novascotia.ca/finance/statistics/archive_news.asp?id=16662&dg=&df=&dto=0&dti=36
He, W., Goodkind, D., & Kowal, P. (2016). An aging world: 2015. International Population Reports. U.S. Census Bureau.
Hinze, S. W., Lin, J., & Andersson, T. E. (2012). Can we capture the intersections? Older black women, education, and health. Women’s Health Issues, 22, e91-e98.
Levy, B. (2009). Stereotype embodiment: A psychosocial approach to aging. Current Directions in Psychological Science, 18, 332-336.
Nelson, T. D. (2016). Promoting healthy aging by confronting ageism. American Psychologist, 71(4), 276-282.
Quinn, J. F., & Cahill, K. E. (2016). The new world of retirement income security in America. American Psychologist, 71(4), 321-333.
Statistics Canada (September 2017). Dictionary, Census of Population, 2016, Market basket measure (MBM). https://www12.statcan.gc.ca/census-recensement/2016/ref/dict/pop165-eng.cfm
Youdin, R. (2016). Psychology of Aging 101. New York: Springer Publishing.
World Health Organization. “Global report on ageism.” (2021).
Media Attributions
- Screen Shot 2022-12-20 at 10.13.43 AM
- Screen Shot 2022-12-20 at 10.19.39 AM
