14 Chapter 13: Mental Health and Aging
Tracy Everitt; Megan Davies; and Laurie Wadsworth
Chapter 13 Learning Objectives
At the conclusion of this chapter, students will be able to:
Learning Objectives
- Understand the risk factors for mental health issues among older adults.
- Describe the impact of depression on older adults.
- Identify the common types of depression that impact older adults.
- Identify care, treatment and prevention strategies for older adults with depression.
- Understand how depression can affect one’s nutrition, especially throughout older age.
- Identify the diagnostic criteria for depression according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
- Understand how anxiety affects older adults, the risk factors, diagnostic criteria, impact, types, treatment, and management regimes.
- Understand how depression affects older adults, the risk factors, diagnostic criteria, impact, types, treatment, and management regimes.
- Identify the medications available for depression and anxiety and potential impacts on nutritional intake and nutritional status.
- Describe strategies and interventions to prevent mental health issues among older adults.
Introduction
Globally, the population is aging. Older adults make important contributions to society as family members, volunteers, and active participants in the workforce. Older adults also face unique physical and mental health challenges. While most have good mental health, many older adults are at risk of developing mental disorders, neurological disorders, or substance use problems. Mental health problems are under-identified by healthcare professionals and older adults themselves, and the stigma surrounding these conditions may make people reluctant to seek help. Addressing mental health illness can be difficult but is incredibly important in promoting healthy and active aging.
13.1 Risk Factors for Mental Health Problems Among Older Adults
There are multiple risk factors for mental health illness at any life stage. Older people may experience similar life stressors as younger adults, as well as those more common in later life. For example, older adults may experience reduced mobility, chronic pain, frailty or other health problems requiring some form of medical or long-term care. In addition, older people are more likely to experience events such as bereavement or a drop in socioeconomic status with retirement. All these stressors can result in isolation, loneliness, or psychological distress in older people.
Mental health illness has an impact on physical health and vice versa. For example, older adults with physical health conditions such as heart disease have higher rates of depression than healthy people. Additionally, untreated depression in someone with heart disease can negatively affect health outcomes.
Insufficient income is a risk factor for poor mental health among older adults. Rates of mood disorders, anxiety, and suicidal thoughts are all higher among seniors aged 65+ in the lowest income quintiles. This can be seen visually in Figures 13.1.1-13.1.3.
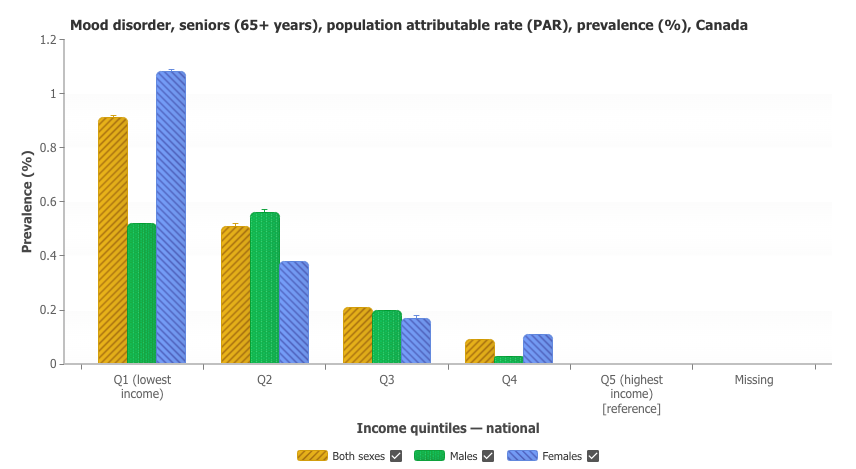
Figure 13.1.1: The prevalence of health inequalities surrounding mental illness and suicide (specifically mood disorder) among seniors (65+ years), contrasted with national income quintiles.

Figure 13.1.2: The prevalence of health inequalities surrounding mental illness and suicide (specifically anxiety disorder) among seniors (65+ years), contrasted with national income quintiles.
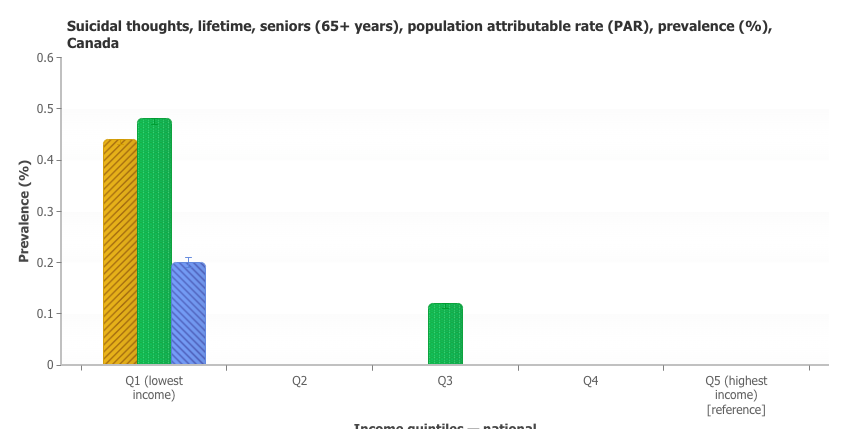
Figure 13.1.3: The prevalence of health inequalities surrounding mental illness and suicide (specifically suicidal thoughts) among seniors (65+ years), contrasted with national income quintiles.
13.2 Depression Among Older Adults
Everyone needs social connections to survive and thrive. But as people age, they often find themselves spending more time alone. Studies show that loneliness and social isolation are associated with higher rates of depression – one of the most common mental health problems among older adults. Depression is a serious mood disorder that can affect how a person feels, acts and thinks. Depression can cause great suffering and can lead to impaired functioning in daily life. Depression is both underdiagnosed and undertreated in primary care settings. Symptoms are often overlooked and untreated because they occur concurrently with other health problems older adults encounter. Older adults often believe that their feelings are due to grief or a medical diagnosis, so they do not seek help, whereas this is treatable.
Depression can have a greater impact on health status than those dealing with chronic physical conditions such as lung disease, hypertension, or diabetes. Depression also increases the perception of poor health, the utilization of health care services, and costs.
Signs and Symptoms of Depression
It’s not always easy to spot someone experiencing depression. Depression presents uniquely amongst people and can vary by life stage. For some older adults with depression, sadness is not their main symptom (NIA, 2021). Instead, they could feel numb, lack interest in activities, and be less willing to talk about their feelings. Understanding common symptoms of depression may help with diagnosis.
Symptoms may include:
- Persistent sadness
- Anxiety or feelings of emptiness
- Feelings of hopelessness, guilt, or worthlessness
- Irritability, restlessness, or having trouble sitting still
- A loss of interest in once pleasurable activities, including sex
- Fatigue or decreased energy
- Moving or talking more slowly
- Difficulty concentrating or making decisions
- Changes in eating patterns, unplanned weight changes
- Thoughts of death or suicide.
Anyone who experiences one or several of these signs and symptoms should talk to their doctor, as these could be signs of depression or another health condition. Healthcare providers should assess depression risk during client visits. Research has shown that intervening during primary care visits effectively reduces suicide later in life.
There are simple screening tools that healthcare providers can use to help identify depression or anxiety symptoms among seniors. The Mental Health Commission of Canada released a report in 2006 which focused on transforming mental health, mental illness, and addiction services in Canada. Chapter 7 (pp. 157-170) focuses on seniors.
The full report: Mental Health Commission Canada
Diagnosis of Depression Disorders
The Diagnostic and Statistical Manual of Mental Disorders (DSM) provides diagnostic criteria for mental health disorders. The DSM-5 outlines the following criteria to make a diagnosis of depression. Major depressive disorder is characterized by discrete episodes of at least 2 weeks’ duration involving clear changes in affect, cognition, and neurovegetative functions and inter-episode remissions (American Psychiatric Association, 2013).
Consideration should be given to the difference between normal sadness and grief from a major depressive episode. Bereavement may induce great suffering, but it does not typically induce an episode of major depressive disorder. When they do occur together, the depressive symptoms and functional impairment tend to be more severe (Amercian Psychiatric Association, 2013). Bereavement-related major depressive episodes tend to occur in persons with other vulnerabilities to depressive disorders. A more chronic form of depression, persistent depressive disorder, can be diagnosed when the mood disturbance continues for at least 2 years in adults or 1 year in children.
The diagnosis of major depressive disorder requires 5 or more symptoms, as seen in Table 13.2.1, during the same 2-week period that represent a change from previous functioning with at least one symptom being depressed mood or loss of interest of pleasure.
Table 13.2.1: The diagnostic criteria for depressive disorders adapted from the Diagnostic and statistical manual of mental disorders: DSM-5.
| Diagnostic Criteria for Depression | |
|
A.
|
Severe recurrent temper outbursts manifested verbally and/or behaviorally that are grossly out of proportion in intensity or duration to the situation or provocation.
|
|
B.
|
The temper outbursts are inconsistent with developmental level.
|
|
C.
|
The temper outbursts occur, on average, three or more times per week.
|
|
D.
|
The mood between temper outbursts is persistently irritable or angry most of the day, nearly every day, and is observable by others.
|
|
E.
|
Criteria A and D have been present for 12 or more months. Throughout that time, the individual has not had a period lasting 3 or more consecutive months without all of the symptoms in Criteria A-D.
|
|
F.
|
Criteria A and D are present in at least two of three settings and are severe in at least one of these.
|
|
G.
|
The diagnosis should not be made for the first time before age 6 years or after age 18 years.
|
|
H.
|
By history or observation, the age at onset of Criteria A-E is before 10 years.
|
|
I.
|
There has never been a distinct period lasting more than 1 day during in which the full symptoms criteria, except duration, for a manic or hypomanic episode have been met.
|
|
J.
|
The behaviors do not occur exclusively during an episode of major depressive disorder and are not better explained by another mental disorder (e.g., autism spectrum disorder, posttraumatic stress disorder, separation anxiety disorder, persistent depressive disorder).
|
Source: (American Psychiatric Association, 2013).
To receive a diagnosis of depression. These symptoms must cause the individual clinically significant distress or impairment in social, occupational, or other important areas of functioning. The symptoms must also not be a result of substance abuse or another medical conditions.
The latest edition of Diagnostic and Statistical Manual of Mental Disorders (DSM), the DSM-5 added two specifiers to further classify diagnosis:
With Mixed Features: This specifier allows for the presence of manic symptoms as part of the depression diagnosis in patients who do not meet the full criteria for a manic episode.
With Anxious Distress: the presence of anxiety in patients may affect prognosis, treatment options, and the patient’s response to them. Clinicians will need to assess whether or not the individual experiencing depression also presents with anxious distress.
Source: (American Psychiatric Association, 2013).
There are several types of depression that older adults may experience:
Major Depressive Disorder – Requires two or more major depressive episodes. Includes symptoms lasting at least two weeks that interfere with a person’s ability to perform daily tasks.
Persistent Depressive Disorder (Dysthymia) – a depressed mood that lasts more than two years, but the person may still be able to perform daily tasks, unlike someone with Major Depressive Disorder. Depressed mood most of the day for more days than not, for at least 2 years, and the presence of two or more diagnostic symptoms that cause clinically significant impairment in social, work, or other important areas of functioning.
Substance/Medication-Induced Depressive Disorder – depression related to the use of substances, like alcohol or pain medication. This disorder is defined as a prominent and persistent disturbance of mood that is judged to be due to the direct psychological effects of a substance. Usually only presents either during intoxication from the substance or on withdrawal from the substance.
Depressive Disorder Due to A Medical Condition – depression related to a separate illness, like heart disease or multiple sclerosis. The criteria for diagnosis is similar to Major Depressive Episode or manic episode; however, the full criteria for these diagnoses need not be met. It is important in diagnosis to establish that the depressive symptoms are a direct physiological result of the medical condition, not just a psychological response to a medical problem.
Other forms of depression include psychotic depression, postmenopausal depression, and seasonal affective disorder. Find detailed descriptions of different types of depression from the National Institute of Mental Health at https://www.nimh.nih.gov/
How Depression Affects Nutrition
Depression can impact the way we eat or view food. When someone is depressed, it can cause poor appetite, skipping meals, and a desire for sweet foods (Rao et al., 2008). Depression can also lead to anxious eating and weight gain. Often people who are depressed make choices that further contribute to their disorder. If depression is not treated it can lead to further health problems, specifically ones linked to their poor diet, malnutrition, and weight loss (Roa et al., 2008).
Depression in Adults with Dementia or Alzheimer’s
Dementia and Alzheimer’s often cause the same symptoms as depression. In addition, suicide is higher in people with dementia. People with dementia need support to help them cope with their diagnosis and possible depression (National Institute of Aging, 2021).
Treatment and Prevention Strategies
Depression is serious, treatments are available to help, and most people improve with treatment. Counselling, medication, or other forms of treatment can be helpful. Health providers can help by recognizing the signs and symptoms and helping older people find appropriate support if mental health concerns arise. Addressing other issues can be supportive such as preventing and managing age-associated chronic diseases, including mental, neurological and substance use disorders.
A healthy lifestyle can help to manage and prevent depression. Physical activity is known to produce endorphins that can elevate one’s mood. Being physically active, eating a healthy balanced diet, getting seven to nine hours of sleep each night, staying in touch with friends and family, and participating in enjoyable activities promote mental health. Anyone experiencing symptoms of depression should inform friends, family, and their physician to optimize support.
Family and friends can support an older person with depression by encouraging them to seek medical treatment and supporting them in following the doctor’s treatment plan. Support people can help set up medical appointments or accompany the person to the doctor’s office or a support group. Friends and family can encourage participation in activities the person enjoys. Each person’s experience is unique, so individualizing a plan with the person’s input is important.
13.3 Anxiety Among Older Adults
Anxiety is a natural response to many life stressors, such as meeting new people, speaking in public, or getting lost in an unfamiliar environment. When these feelings of nervousness become overwhelming and make everyday life more difficult, it may be a sign of an anxiety disorder. Anxiety disorders affect nearly 4% of older adults worldwide – and those are only cases that are recognized and diagnosed (NCOA, 2022). Many cases go underdiagnosed due to misconceptions about mental illness. Severe anxiety is not an inevitable part of aging. With the proper treatment, older adults can find relief from their symptoms and return to their normal lives.
There are a few different types of anxiety. Generalized anxiety disorder is the most common form of anxiety where an individual experiences persistent and excessive anxiety and worry towards various domains, including work and school performance. In addition, the individual experiences physical symptoms, including restlessness or feeling on the edge; being easily fatigued; difficult concentrating or mind going blank; irritability; muscle tension; sleep disturbances (American Psychiatric Association, 2013). Individuals with specific phobia are fearful or anxious about or avoidant of circumscribed objects or situations (American Psychiatric Association, 2013). Social anxiety disorder causes an individual to be fearful or anxious about or avoidant of social interactions and situations that involve the possibility of being scrutinized (e.g., meeting new people, uncomfortable situations such as when the individual must perform in front of others, etc.) (American Psychiatric Association, 2013). Panic disorder causes an individual to experience recurrent unexpected panic attacks and is persistently concerned or worried about having more panic attacks or changes in their behavior due to these panic attacks (American Psychiatric Association, 2013). Individuals with agoraphobia are fearful and anxious in many different situations, and the diagnostic criteria require symptoms in two or more of the following: using public transportation, being in open spaces, being in enclosed places, standing in line or being in a crowd, or being outside of the home alone in other situations (American Psychiatric Association, 2013). Substance/medication-induced anxiety disorder involves anxiety due to substance intoxication or withdrawal or to a medication treatment (Amercian Psychiatric Association, 2013).
Individuals with anxiety may be more likely to have suicidal thoughts, attempt suicide, and die by suicide than those without anxiety. Panic disorder, generalized anxiety disorder, and specific phobia have been identified as the anxiety disorders most strongly associated with a transition from suicidal thoughts to suicide attempt (American Psychiatric Association, 2013).
Risk Factors for Anxiety in Older Adults
Anxiety can be caused by a multitude of triggers, and sometimes even by nothing at all. It can stem from environmental, situational, and genetic factors. While it is difficult to pinpoint a direct cause of anxiety disorders, we do know some common risk factors for older adults:
- Stressful life events
- Limited physical mobility
- Loss of independence
- Financial insecurity
- Sleep disturbances
- Chronic health conditions
- Side effects of medications
- Misuse/abuse of alcohol or prescription medications
- Trauma from childhood
Source: (Anxiety and older adults: A guide to getting the relief you need, 2022).
Mental health professionals look for factors like excessive, hindering worry paired with a variety of physical symptoms, then use proven diagnostic assessments to make a diagnosis and rule out other possibilities. The DSM-5 outlines specific criteria to help professionals diagnose GAD.
Diagnosis of Generalized Anxiety Disorder
When assessing for GAD, clinical professionals are looking for the diagnostic criteria listed in Table 13.3.1.
Table 13.3.1. Diagnostic criteria for generalized anxiety disorder.
| Diagnostic Criteria for Generalized Anxiety Disorder | |
|
A.
|
Excessive anxiety and worry, occurring more days than not for at least 6 months, about several events or activities.
|
|
B.
|
The individual finds it difficult to control the worry.
|
|
C.
|
The anxiety and worry are associated with three (or more) of the following 6 symptoms (with some of the symptoms been present for more days than not for the past 6 months):
|
|
D.
|
The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
|
|
E.
|
The disturbance is not attributable to the physiological effects of a substance or another medical condition.
|
|
F.
|
The disturbance is not better explained by another mental disorder (I.e., obsessive-compulsive disorder, separation anxiety disorder, post-traumatic stress disorder, body dysmorphic disorder, having a serious illness, schizophrenia or delusional disorder).
|
Source: (American Psychiatric Association, 2013)
The anxiety, worry, and other symptoms of GAD make it hard to carry out day-to-day activities and responsibilities. To diagnose GAD, these symptoms also must be unrelated to any other medical conditions and cannot be explained by a different mental disorder or by the effect of substance abuse, including prescription medication, alcohol, or recreational drugs.
Treatment and Management of Anxiety in Older Adults
Stigma and lack of knowledge surrounding mental illness often result in older adults not reaching out for the help they need and deserve. Anxiety disorders are typically treated with a combination of medication and talk therapy, but one or the other can be used by itself as well.
Talk therapy is one-on-one counselling with a therapist/counsellor. The two most common forms are exposure therapy and cognitive behavioural therapy (CBT). Exposure therapy involves facing a fear to increase confidence. Cognitive behavioural therapy (CBT) involves identifying harmful thoughts and behaviours and finding ways to modify or change them.
Medications help ease anxiety and are often used in combination with talk therapy. Anti-anxiety medications and antidepressants are the most common types of medications used.
On top of medical treatments for anxiety disorders, certain lifestyle changes can also help lesson feelings of anxiety:
- Talking about feelings with trusted peers can help alleviate anxiety
- Practicing mindfulness, such as doing yoga or meditating, can promote relaxation
- It can be challenging; however, getting sufficient sleep can help prevent anxiety caused by lack of sleep. Strategies to support optimal sleep include creating a quiet, dark, relaxing, comfortable sleep environment, avoiding large meals, and limiting caffeine and alcohol.
Medications for Depression and Anxiety
The following section describes medications used for anxiety and depression.
Selective serotonin reuptake inhibitors (SSRIs)
SSRIs are designed to treat depression and anxiety disorders. They block serotonin from being reabsorbed by the brain, increasing serotonin levels and mood. The generic (and brand names) of the SSRIs include Fluoxetine (Prozac), Citalopram (Celexa), Escitalopram (Lexapro, Cipralex), and Sertraline (Zoloft).
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
SNRIs are designed to treat depression and anxiety. They work by increasing the level of active neurotransmitter by blocking serotonin and norepinephrine from reabsorbing back into the nerve cells that released them. The resultant increased levels of serotonin and norepinephrine increase mood. The generic (and brand names) of SNRIs include Venlafaxine (Effexor), Duloxetine (Cymblata), Desvenlafaxine (Pristiq).
Benzodiazepines
Benzodiazepines are used for short-term treatment of anxiety and are often added to an existing medication regimen in treating resistant anxiety. They have sedative properties due to their mechanism of action. Benzodiazepines enhance the GABA (gamma-aminobutyric acid) neurotransmitter, which results in a calming effect. They are potentially addictive, and overuse can lead to dependence and/or abuse. The generic (and brand names) of benzodiazepines include Lorazepam (Ativan), and Alprazolam (Xanax).
Tricyclic Antidepressants
Tricyclic antidepressants were originally designed to treat depression but are commonly used to treat anxiety due to concerns about the long-term use of benzodiazepines. They work by blocking the reabsorption of serotonin and norepinephrine, which increases levels in the synaptic cleft (gap between the pre-and post-synaptic cells), resulting in an increased mood. Tricyclic antidepressants include Amitriptyline (brand name no longer available in Canada), Clomipramine (Anafranil, also used for obsessive compulsive disorder), Nortriptyline (Aventyl), and Doxepin (Silenor).
Table 13.2.1. Summary of medications to treat depression and anxiety.
|
Class
|
Mechanism
|
Side Effects
|
|
Selective serotonin reuptake inhibitors (SSRIs)
|
Blocks reabsorption/reuptake of serotonin by nerve cells in the brain, increasing the amount of serotonin available and increasing mood.
|
Nausea, vomiting, weight gain, dry mouth
|
|
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
|
Block reuptake to increase levels of serotonin and norepinephrine so they stay in the synaptic cleft longer, increasing mood.
|
Nausea, fatigue, loss of appetite. High doses can increase blood pressure
|
|
Benzodiazepines
|
Enhances GABA neurotransmitter which results in a calming effect
|
Constipation, dry mouth, nausea, and vomiting
|
|
Tricyclic Antidepressants
|
Block reabsorption/reuptake of serotonin and norepinephrine increases synaptic cleft levels, increasing mood.
|
Dry mouth, constipation, problems urinating, weight gain
|
Here are some recommendations to help treat some of these common side effects of medications.
| Side Effect | Recommendation |
| Nausea/Vomiting |
|
| Fatigue |
|
| Weight Gain |
|
| Dry Mouth |
|
| Constipation |
|
13.4 Strategies to Help Improve Mental Health
Older adults often face many changes and sources of stress, such as loss of strength, illness, children moving away from home, and life changes due to retirement. The key to coping with changes include healthy lifestyle habits promoting active aging, planning for life changes, strengthening relationships with surviving friends and family, and maintaining interest and involvement with life. Healthy coping strategies and support from friends, families, communities, and the government can help strengthen and promote mental health in older adults. The Mental Health Commission of Canada has specific strategies designed to address mental health issues in older adults: https://mentalhealthcommission.ca/what-we-do/older-adults/
Dealing with Bereavement
As adults age, they will likely experience the loss of loved ones more often, leading to periods of grief. Bereavement refers to the outward expression of grief. It is important that older adults learn ways of coping with grief during these difficult times. Losing someone to death can feel like being wounded and requires time to heal. If adults do not allow themselves to go through the grieving process, they may store problems for a delayed reaction. It is important to accept the range of emotions experienced. Tears, anger, and guilt are all normal reactions and ways of moving through grief may change from one loss to another. Family and friends can provide support during these times. Mourning is an expression of loss that reflects personal and cultural beliefs about the meaning of death. Mourning with friends and family can help older adults find peace. Ultimately, having support through times of loss helps to support mental health.
Dealing with Loneliness
Everyone requires time alone, but being alone against one’s will can be very painful, causing someone to risk losing their sense of purpose and self-worth. Changing life circumstances can contribute to loneliness, and finding ways to cope with change is important. Adaptive strategies may include staying active and looking for new social contacts, joining community support programs, volunteering part-time or spending time with grandchildren. Socializing can provide opportunities for making new friends, allowing older adults to try new activities that can contribute to healthy and active aging.
Dealing with Retirement
Retirement can be a major source of stress for older adults because their job can be an important part of their life and contribute to self-worth and a sense of identity. Retirement stress may be greater if they have been forced to retire due to health issues, family obligations or changes in work circumstances. Retirees may miss daily contact with friends from work. However, retirement can be one of the best times of one’s life. Retirement can provide an opportunity to do activities, use skills, reconnect with others, or be involved with meaningful volunteer work. Work can interfere with relationships; therefore, revisiting these relationships can be rewarding for retirees. Enriching one’s life by renewing contacts with family members and old friends can be important. Renewing interest in hobbies and other enjoyable activities can be uplifting for an older person.
13.5 Health Promotion
Older adults’ mental health can be improved by promoting active and healthy aging. This is supported by living conditions and environments that support well-being and allow people to lead healthy lives.
Resources to support healthy aging, include:
- Security and freedom
- Adequate housing and supportive housing policy
- Social support for older people and their caregivers
- Health and social programs targeted at vulnerable groups such as those who live alone and rural populations or who suffer from a chronic or relapsing mental or physical illness
- Programs to prevent and deal with elder abuse
- Community development programs.
Supportive environments promote mental health in older adults. Strategies for identifying mental health conditions and intervening such as regular screening of older adults in community or in LTC is also an important form of health promotion. This could help identify some short-term anxieties that could be better managed, such as those that often accompany grief.
Mental Health Care in the Community
Good general health and social care are important for promoting older people’s health, preventing disease, and managing chronic illnesses. All health providers should learn about how to support healthy aging. Effective, community-level primary mental health care for older people is crucial. It is equally important to focus on the long-term care of older adults suffering from mental disorders and provide caregivers with education, training, and support.
For further information on how supportive environments can promote mental health wellness among older adults, please read the WHO Age-Friendly Cities Framework
Questions:
- What are some local examples of accessible and affordable health services for older adults?
- In your opinion, what are some of the most important strategies to address barriers to mental health well-being in Canada?
This chapter is adapted from ‘Lifespan Development’ by Lumen Learning: https://pressbooks.nscc.ca/lumenlife/
Creative Commons Attribution: BY
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5 (Vol. 5, No. 5). Washington, DC: American psychiatric association.
Antidepressant Medications. (n.d.). CAMH. Retrieved April 13, 2023, from https://www.camh.ca/en/health-info/mental-illness-and-addiction-index/antidepressant-medications
Antidepressants: Get tips to cope with side effects. (n.d.). Mayo Clinic. Retrieved April 13, 2023, from https://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20049305
Benzodiazepines: Canada : eMentalHealth.ca. (n.d.). EMentalHealth.ca Resource Directory. Retrieved April 13, 2023, from https://www.ementalhealth.ca/Canada/Benzodiazepines/index.php?m=article&ID=20910
Canadian Mental Health Association (2022). “Aging and mental health.” Retrieved from https://toronto.cmha.ca/documents/aging-and-mental-health/
Cooper, Rachel. Diagnosing the Diagnostic and Statistical Manual of Mental Disorders : Fifth Edition, Taylor & Francis Group, 2014. ProQuest Ebook Central, https://ebookcentral.proquest.com/lib/stfx/detail.action?docID=1684462.
Glasofer, D. (2022, April). How is generalized anxiety disorder diagnosed using the DSM-5-TR? Verywell Mind. Retrieved December 19, 2022, from https://www.verywellmind.com/dsm-5-criteria-for-generalized-anxiety-disorder-1393147
National Council on Aging (2022, April 22). Anxiety and older adults: a guide to getting the relief you need. Retrieved from https://www.ncoa.org/article/anxiety-and-older-adults-a-guide-to-getting-the-relief-you-need
National Institute on Aging (2018, June). “Impact of the DSM-IV to DSM-5 changes on the national survey on drug use and health.” Substance Abuse and Mental Health Services Administration. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK519704/table/ch3.t15/
National Institue on Aging (2021). “Depression in older adults.” Retrieved from https://www.nia.nih.gov/health/depression-and-older-adults \
PSYCOM (2018, July 24). Depression definition and DSM-5 diagnostic criteria. Retrieved December 19, 2022, from https://www.psycom.net/depression/major-depressive-disorder/dsm-5-depression-criteria
World Health Organization (2017). “Mental health of older adults.” Retrieved from https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults
Media Attributions
- Screen Shot 2022-12-22 at 11.15.17 AM
- Screen Shot 2022-12-22 at 11.15.31 AM
- Screen Shot 2022-12-22 at 11.16.03 AM
