7 Chapter 6: Body Composition Changes
Tracy Everitt; Brittany Yantha; Megan Davies; and Shannon Roode
Chapter 6 Learning Objectives
At the conclusion of this chapter, students will be able to:
Learning Objectives
- Describe the connection between body weight and health status.
- Explain the concern towards obesity in older adults.
- Identify interventions to aid in health weight loss.
- Describe the condition of anorexia of aging and why this is a concern for older adults.
- Describe sarcopenia along with the cause and treatment.
- Describe cachexia, along with the cause of treatment.
- Illustrate why older adults have an increased risk of fragility and identify those at higher risk.
Introduction
Adequate nutrition is essential for cell and tissue repair to ensure older adults maintain health and continue engaging in daily activities. A healthy diet supports physical and cognitive ability, bone health, eye health, vascular function, and the immune system. As people age, their dietary and nutritional needs change. Adequate nutrition helps to support the changes that occur through the aging process, promotes well-being and prevents frailty. Adapting to changes and overcoming challenges that arise supports optimal well-being.
6.1 Body Weight and Health Status in Older Adults
The foods consumed throughout the lifespan influence health as people age. The aim of healthy aging is to increase years of life and, more importantly, to extend healthy active years. Good nutrition and regular physical activity can help those live longer and healthier. Conversely, poor nutrition and a lack of exercise can shorten one‘s life and lead to medical problems. Changes that go along with aging can make following dietary recommendations challenging. For instance, physiological changes can affect taste and smell, appetite, and dental and chewing functions, while changes in family dynamics can lead to less support in overcoming these challenges. Food intake influences body composition, contributing to weight status – being overweight or underweight – both of which can contribute to health concerns.
Obesity
Some nutrients may be deficient in the diets of older adults, while others may be consumed in excess. Extras calories, for example, can lead to overnutrition and contribute to obesity and chronic conditions. Obesity is a complex chronic disease in which dysfunctional fat (fat with metabolic processes contributing to chronic inflammation or metabolic syndrome) or excess body fat impairs health, increases long-term medical complications and reduces life span (Twells, Janssen & Kuk, 2020). Health-related quality of life can be lower for individuals living with obesity compared to the general population due to problems with pain and discomfort, reduced mobility and impacts on mental health, such as increased depression and anxiety. In epidemiological research, obesity is often determined using the body mass index (BMI), calculated as weight in kilograms divided by height in meters squared (kg/m2). Obesity is defined as a BMI greater than or equal to 30 kg/m2 and further divided into subgroups: Class I: BMI 30–34.9 kg/m2, Class II: BMI 35–39.9 kg/m2 and Class III: BMI ≥ 40 kg/m2. The term severe obesity is used for individuals with a BMI ≥ 35 kg/m2 (Twells, Janssen & Kuk, 2020). Although BMI has limitations, it is commonly used to estimate the health risks associated with excess body weight due to ease of measurement. Other anthropometric measures such as waist circumference, waist-to-hip ratio and skinfold measures can detail the degree of abdominal adiposity – the weight distribution pattern associated with increased health risk.
Obesity among older adults is rising (Wang, et al., 2017). Obesity is a concern for older adults because it contributes to a higher risk for degenerative diseases and age-related health and physical function declines, leading to increased dependence, disability, and morbidity (Berstein & Munoz, 2012). For older adults who are overweight or obese, dietary changes to promote weight loss should be combined with an exercise program to preserve muscle mass. Dieting reduces both muscle and fat, exacerbating muscle mass loss due to aging. Although weight loss among older adults can be beneficial, it is best to be cautious because weight loss in older adults can decrease muscle, and this is negatively correlated with functional capacity.
Canadian clinical practice guidelines state that all individuals, regardless of body size or composition, would benefit from adopting a healthy, well-balanced eating pattern and engaging in regular physical activity (Wharton et al., 2020). Weight loss and weight loss maintenance require a long-term reduction in caloric intake. Long-term adherence to a healthy eating pattern, personalized to meet individual values and preferences while fulfilling nutritional needs and treatment goals, is important in managing health and weight. The weight at which the body stabilizes when engaging in healthy behaviours can be referred to as the “best weight”; this may not be an “ideal” weight on the BMI scale. Achieving an “ideal” BMI may be very difficult. Because obesity is a chronic disease, patient-provider collaboration can help to manage it in the long term. Talking with patients and agreeing on realistic expectations, using person-centered treatments, and developing sustainable goals for behaviour change and health outcomes can support healthy weight management in older adults.
The Anorexia of Aging
Although much attention is placed on the impact of obesity on health, being underweight can also be a significant problem. A condition known as anorexia of aging is characterized by poor food intake, resulting in significant and unhealthy weight loss, leading to a higher risk for immune deficiency, frequent falls, muscle loss, and cognitive deficits. As a healthcare provider, it is important to examine the causes of anorexia of aging, which can vary from one individual to another. Understanding why some older adults eat less as they age can help healthcare professionals assess the risk factors associated with this condition. Complex mechanisms are involved in the age-related loss of appetite or decreased food intake. Smell and taste play a key role in making eating and drinking enjoyable. These senses decrease with age, contributing to diminished food intake. Sensory changes can also negatively impact the types of food eaten, as pre-packaged and processed foods are higher in sodium and sugar and can be more enjoyable for older adults with reduced smell and taste (MacIntosh, 2000). Hormonal changes throughout aging can also contribute to decreased food intake. Higher levels of leptin and insulin, which act as satiety hormones, may accelerate the development of anorexia in seniors. The hunger hormone, ghrelin, is affected by increases in circulating leptin and insulin, leading to decreased food intake (Di Francesco, et al., 2007). Changes in gastrointestinal function and abnormalities in gastric motility may cause early satiation in older adults. Delayed and slower gastric emptying may decrease the appetite and food intake, modifying the body‘s satiety signals (MacIntosh, 2000). Chronic, low-grade inflammation that tends to occur as a person ages is common in older adults and may affect appetite (Laviano, et al., 2005).
Physical and social factors and medications may contribute to anorexia of aging. Physical impairments can cause mobility limitations that, in turn, could create problems such as eating by oneself or difficulty getting food (Landi, et al., 2015). Poor dentition and ill-fitting dentures may limit the type and quantity of food consumed (Mir, et al., 2013). Older adults may take many prescriptions as well as over-the-counter medications. Many of these medications can cause malabsorption, gastrointestinal disorders, loss of appetite and reduced food intake. The risk of drug-induced anorexia is further increased by polypharmacy, due to increased risk of drug-drug interactions and gastrointestinal problems (Onder, et al., 2014). Other risk factors associated with anorexia of aging include social factors. Socioeconomic status, for example, can impact food access and social isolation and living alone is also associated with reduced appetite and energy intake (De Castro, 1993).
Anorexia of aging is associated with several serious health impacts. Malnutrition is common among those experiencing anorexia due to suboptimal intake of nutrients such as proteins and vitamins (Landi, et al., 2015).
Nutrition interventions for anorexia of aging should focus primarily on a healthy diet. Remedies can include increasing the frequency and variety of meals and adding healthy, high-calorie foods (such as nuts, potatoes, whole-grain pasta, and avocados). Flavour enhancements with meals and oral nutrition supplements between meals may help improve calorie intake. Environmental adaptations can also be useful for older adults as these interventions prevent social isolation.
Unintentional Weight Loss
Rapid involuntary weight loss and low body mass index (BMI) in older adults indicate underlying disease and are associated with mortality. There are three known categories of risk factors for unintentional weight loss: physiologic, psychological, and socioeconomic. Physiologic risk factors that can lead to unintentional weight loss include decreased appetite, oral health concerns, sensory impairment, disease, and functional deficits. Psychological risk factors include depression, dementia, cognitive impairment, and mental illness. Socioeconomic factors such as social isolation, food insecurity, and lack of caregiver support can increase the risk of unintentional weight loss. Unintended weight loss is often associated with poor health outcomes and is a marker for deteriorating well-being. Unexplained weight loss is treated by identifying and addressing the underlying condition.
6.2 Sarcopenia
Loss of skeletal muscle mass and muscle strength is a prominent feature of age-related changes in body composition. Sarcopenia is defined as poor function due to losing muscle mass or muscle strength and function (Morley, 2017). This condition is associated with physical disability, impaired mobility, a higher risk of falls, frailty, cognitive dysfunction, and other age-related conditions. Sarcopenia is estimated to affect 8% to 40% of adults above 60 and approximately 50% of those aged >75 years (Bernstein & Munoz, 2012). Sarcopenia is a complex condition resulting from several changes that occur with aging; however, a sedentary lifestyle and nutritional inadequacies are primary contributors to the onset of sarcopenic symptoms. Resistance exercise and adequate protein intake represent the most important therapeutic modalities to address sarcopenia. Regularly consuming high-quality proteins can be challenging for older adults with limited resources, reduced appetite, and physical and environmental limitations. The role of dietary protein in preventing sarcopenia remains unclear; however, a protein intake moderately greater than the Recommended Dietary Allowance may be beneficial to enhance muscle protein anabolism and reduce progressive loss of muscle mass with age.
Sarcopenic Obesity
Sarcopenic obesity is the coexistence of age-related loss of skeletal mass and strength with excess body fat. The prevalence of sarcopenic obesity has been found to increase with advancing age and increases the risk for adverse outcomes and functional impairment. The Canadian Longitudinal Study on Aging (n= 11,803) found that sarcopenic obesity ranged from 0.1-85.3% in males and from 0-80.4% in females. Identifying factors of sarcopenic obesity include the deterioration of muscle composition and quality in combination with an increase in overall fat mass.The hand-grip strength test can help identify muscular strength and indicate whether sarcopenia is present. Excess energy intake, physical inactivity, low-grade inflammation, insulin resistance, and changes in hormone levels can all lead to sarcopenic obesity (Bernstein & Munox, 2012).
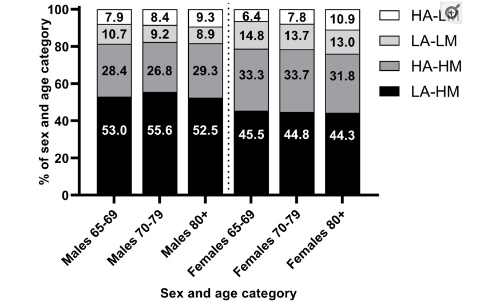
Figure 6.2.1: Prevalence of different body composition phenotypes by sex and age group. HA, high adiposity; LM, low muscularity; LA, low adiposity; LM, low muscularity.
Figure 6.2.1 is a visual representation of common body composition phenotypes that are observed among older adults in Canada. There is a lot of variability in the body composition of older adults as shown in Figure 6.2.1. The most prevalent body composition phenotype is low adiposity and high muscularity, followed by high adiposity and high muscularity (Purcell et al., 2021). High adiposity and low muscularity (sarcopenic obesity) was present only in a minority of individuals, and the prevalence of low adiposity and low muscle across all subgroups was higher than the prevalence of underweight. Ultimately, the prevalence of sarcopenic obesity varied greatly and was frequently associated with low hand–grip strength (Purcell et al., 2021).
6.3 Cachexia
Chronic disease and illness are more common among the aging population due to lower muscle mass, inflammation, and oxidative stress. Those experiencing chronic disease or illness may develop a syndrome called cachexia. Cachexia is a complex metabolic syndrome associated with underlying illness and characterized by muscle loss with or without fat mass loss (Evans, et al., 2008). Weight loss and muscle wasting are important in the pathophysiology of cachexia and can be a major cause of fatigue in older adults. Chronic disease can cause the body to be hypermetabolic and lead to unintentional weight loss or wasting. For example, malnutrition is common in cancer patients and can occur throughout a patient‘s disease. Key components of treating cancer cachexia include identifying and managing symptoms and addressing barriers to adequate oral intake. Those experiencing cachexia may be supported through nutrition therapies such as increased protein and caloric intake to combat muscle wasting.
6.4 Frailty
The term ‘nutritional frailty’ has been used to describe a state commonly seen in vulnerable older adults, characterized by sudden significant weight loss and loss of muscle mass and strength or an essential loss of physiologic reserves, making the individual susceptible to disability. Nutritional problems and increased risk of malnutrition contribute to frailty via the culmination of sociologic, biological, and cognitive issues. Frailty is not a specific medical condition like cancer, diabetes, or a disability but is more like a syndrome that results from multiple factors in which an individual may need additional support with activities (Sinha, et al., 2018). As people age, older adults can develop complex health conditions. Multidimensional syndrome of loss of reserves such as energy, physical ability, cognition, and health can give rise to vulnerability in older adults. Frailty puts individuals at an increased risk of functional impairment, falls, hospitalization, long-term care use, and death following stress, such as a minor illness or infection (Sinha et al., 2018). About 10% of community-dwelling older adults are believed to be frail, but more than 40% are at risk of becoming frail (Kojima, 2015).
Since frailty is an evolving concept, the specific factors included in measuring frailty are subject to debate. Some measurements include chronic health conditions, sleep quality, mental health, and disability. While the prevalence of frailty increases with age, it is not necessarily synonymous with age. An Individual’s level of physical fitness, overall health status, and other variables also contribute to their frailty. Factors affecting frailty include chronic conditions and cancer, cardiovascular disease, multi-morbidity, and polypharmacy (Sinha, et al., 2018). Depression may also be a risk factor for frailty. This may be due to the symptoms that correspond with depression or the use of antidepressants, which increases the risk of falls and fractures.
Socioeconomic, demographic, and gender factors appear to contribute to an individual’s level of risk for becoming frail. Women are twice as likely to be diagnosed with frailty, which may be due to lower muscle mass. Having a lower income and being socially isolated are also associated with frailty. Access to secure, stable, and affordable housing can help an individual avoid the adverse outcomes of frailty. Individuals who live in communities with greater levels of neighbourhood deprivation have higher levels of frailty. People with frailty experience low physical activity, low energy levels, slower walking speeds and non-deliberate weight loss. Frailty is associated with a lower quality of life, a higher mortality risk, and more frequent hospitalization, and institutionalization.
Frailty Tools
The definition of frailty remains unclear leading to the creation of many scales to measure, reflecting the uncertainty about the term and its components. Measuring frailty is useful at a clinical and healthcare policy level. Information about frailty helps program planners by identifying the range of services that might be required. Clinically, frailty stratification can help plan interventions or predict a patient’s risk of death or need for institutional care (Rockwood et al., 2005). Because the scales are intended to stratify risk, the ability to predict adverse outcomes serves a common goal.
The Clinical Frailty Scale was developed to be both predictive and easy to use. The 7-point Clinical Frailty Scale is rooted in a theoretical model of fitness and frailty and the importance of function (Rockwood et al., 2005). The Clinical Frailty Scale ranges from 1 (robust health) to 7 (complete functional dependence on others).
The Clinical Frailty Scale
1. Very fit – robust, active, energetic, well-motivated and fit; these people commonly exercise regularly and are in the most fit group for their age
2. Well – without active disease, but less fit than people in category 1
3. Well, with treated comorbid disease – disease symptoms are well controlled compared with those in category 4
4. Apparently vulnerable – although not frankly dependent, these people commonly complain of being “slowed up” or have disease symptoms
5. Mildly frail – with limited dependance on others for instrumental activities of daily living
6. Moderately frail – help is needed with both instrumental and non-instrumental activities of daily living
7. Severely frail – completely dependent on others for the activities of daily living, or terminally ill
Source: (Rockwood et al., 2005)
A link to the Clinical Frailty Scale can be found here: Clinical Frailty Scale.
In a study using the Clinical Frailty Scale, participants with higher scores were older, more likely to be female, were cognitively impaired and incontinent, had impaired mobility and function, and had more comorbid illnesses than those with lower scores.
Maintaining good nutrition as people age is one of the most critical ways to prevent frailty. The Canadian Frailty Network compiled the ‘Avoiding Frailty Shopping List’ as shown in Figure 6.4.2 to help people choose food high in nutrition and low in calories to prevent frailty. As people age, some nutrients such as protein, calcium and vitamin D are critical to keep one’s bones and muscles strong well into old age. Common features of frailty include low grip strength, low energy, slowed waking speed, low physical activity, and/or unintentional weight loss. For further information on what frailty is and how to identify it here is a link to the Canadian Frailty Network.
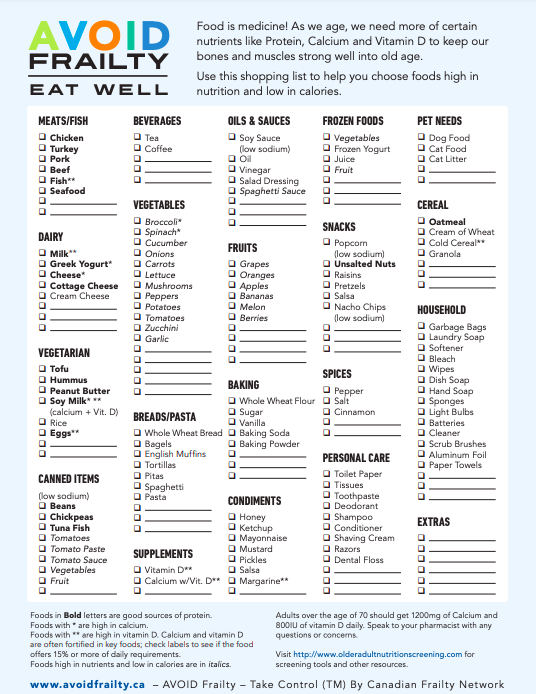
Figure 6.4.2: AVOID Frailty, a printable resource for older adults used to treat and prevent frailty.
Calcium and vitamin D are vital for bone and muscle health. Vitamin D helps with the absorption of calcium and has roles in the nervous, muscle and immune systems (Canadian Frailty Network, n.d.). Protein helps maintain muscle mass, which is important for healthy aging. Meeting nutritional needs is essential for cell and tissue repair to ensure older adults keep healthy and able to do daily activities. Adjusting one‘s eating habits in response to changes that accompany aging can support wellbeing and prevent frailty.
This chapter is adapted from ‘Lifespan Development’ by Lumen Learning: https://pressbooks.nscc.ca/lumenlife/
Creative Commons Attribution: BY
References
Bernstein, M., & Munoz, N. (2012). Position of the Academy of Nutrition and Dietetics: food and nutrition for older adults: promoting health and wellness. Journal of the Academy of Nutrition and Dietetics, 112(8), 1255-1277.
Canadian Frailty Network (n.d.). Diet and nutrition. Retrieved from https://www.cfn-nce.ca/frailty-matters/avoid-frailty/diet-and-nutrition/
Cox, N. J., Ibrahim, K., Sayer, A. A., Robinson, S. M., & Roberts, H. C. (2019). Assessment and treatment of the anorexia of aging: A systematic review. Nutrients, 11(1), 144. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6356473/
De Castro, J.M. Age-related changes in spontaneous food intake and hunger in humans. Appetite 1993, 21, 255–272.
Di Francesco, V.; Fantin, F.; Omizzolo, F.; Residori, L.; Bissoli, L.; Bosello, O.; Zamboni, M. The anorexia of aging. Dig. Dis. 2007, 25, 129–137.
Kojima, G. (2015). Prevalence of Frailty in Nursing Homes: A Systematic Review and Meta-Analysis. JAMDA, 16, 940-945. Retrieved from: https://www.clinicalkey.com/#!/content/playContent/1-s2.0-S1525861015004466?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS1525861015004466%3Fshowall%3Dtrue&referrer=https:%2F%2Fwww.ncbi.nlm.nih.gov%2F
Landi, F., Calvani, R., Tosato, M., Martone, A. M., Ortolani, E., Savera, G., … & Marzetti, E. (2016). Anorexia of aging: risk factors, consequences, and potential treatments. Nutrients, 8(2), 69.
Landi, F.; Lattanzio, F.; Dell’Aquila, G.; Eusebi, P.; Gasperini, B.; Liperoti, R.; Belluigi, A.; Bernabei, R.; Cherubini, A. Prevalence and potentially reversible factors associated with anorexia among older nursing home residents: Results from the ULISSE project. J. Am. Med. Dir. Assoc. 2013, 14, 119–124.
Laviano, A.; Meguid, M.M.; Inui, A.; Muscaritoli, M.; Rossi-Fanelli, F. Therapy insight: Cancer anorexia-cachexia syndrome—When all you can eat is yourself. Nat. Clin. Pract. Oncol. 2005, 2, 158–165.
MacIntosh, C.; Morley, J.E.; Chapman, I.M. The anorexia of aging. Nutrition 2000, 16, 983–995.
Mir, F.; Zafar, F.; Morley, J.E. Anorexia of aging: Can we decrease protein energy undernutrition in the nursing home? J. Am. Med. Dir. Assoc. 2013, 14, 77–79.
Morley, J.E. Pathophysiology of the anorexia of aging. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 27–32.
Onder, G.; Landi, F.; Fusco, D.; Corsonello, A.; Tosato, M.; Battaglia, M.; Mastropaolo, S.; Settanni, S.; Antocicco, M.; Lattanzio, F. Recommendations to prescribe in complex older adults: Results of the Criteria to assess appropriate Medication use among Elderly complex patients (CRIME) project. Drugs Aging 2014, 31, 33–45.
Prado, C. M., Anker, S. D., Coats, A. J., Laviano, A., & von Haehling, S. (2021). Nutrition in the spotlight in cachexia, sarcopenia and muscle: Avoiding the wildfire. Journal of Cachexia, Sarcopenia and Muscle, 12(1), 3.
Rockwood, K., Song, X., MacKnight, C., Bergman, H., Hogan, D. B., McDowell, I., & Mitnitski, A. (2005). A global clinical measure of fitness and frailty in elderly people. Cmaj, 173(5), 489-495.
Sinha, S., McKee, A., Dunning, J., Wong, I., Nicin, M., & Muscedere, J. (2018). We can’t address what we don’t measure consistently: building consensus on frailty in Canada. Natl Institute Ageing, 1-56.
Twells, L., Janssen, I., Kuk, J. (August 4, 2020). Epidemiology of adult obesity. Canadian Adult Obesity Clinical Practise Guidelines, retrieved from https://obesitycanada.ca/guidelines/epidemiology.
Wang, M., Yi, Y., Roebothan, B. et al. (2017). Trajectories of body mass index among Canadian seniors and associated mortality risk. BMC Public Health 17, 929 . https://doi.org/10.1186/s12889-017-4917-0
Wharton, S., Lau, D. C., Vallis, M., Sharma, A. M., Biertho, L., Campbell-Scherer, D., … & Wicklum, S. (2020). Obesity in adults: a clinical practice guideline. Cmaj, 192(31), E875-E891.
Media Attributions
- Screen Shot 2022-12-20 at 4.09.09 PM
- Screen Shot 2022-12-20 at 4.09.53 PM
