Stages of Development
Learning Objectives
By the end of this section, you will be able to:
- Describe the stages of prenatal development
- Identify factors that influence prenatal development
- Explain theories of cognitive and psychosocial development
- Describe the major changes that occur in adolescence
Development from conception into a fully grown human involves major alterations to anatomy, physiology, cognition, and behaviour, and many of these changes follow a predictable, age-based progression. This section will discuss prenatal, infant, child, adolescent, and adult development across three domains: physical, cognitive, and psychosocial.
Prenatal Development
How did you come to be who you are? From beginning as a one-cell structure to your birth, your prenatal development occurred in an orderly and delicate sequence. There are three main stages of prenatal development: germinal, embryonic, and fetal. Let’s explore what happens to the developing baby in each of these stages.
Germinal Stage (Conception–Week 2)
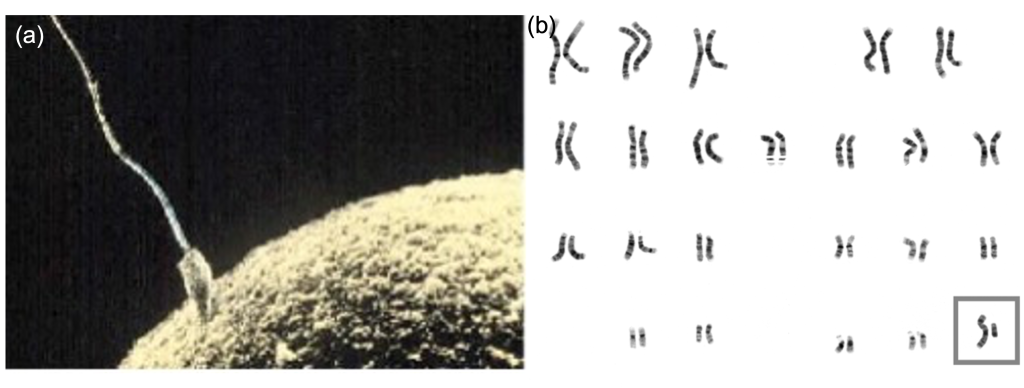
Each biological parent contributes DNA at the moment of conception, when sperm and egg unite to form a single-celled zygote (Figure 4.7). Growth and development of the zygote are guided by these inherited genetic instructions, coded in DNA within 46 chromosomes, 23 from each parent. In mammals, sex is determined by contribution of specific chromosomes, females are typically XX and males are typically XY, so it’s the male parent’s contribution that determines genetic sex, a female parent only has Xs to contribute.
Fetal Stage (Week 8-9 – Onward)
At about nine weeks, the embryo becomes a fetus. At this stage, the fetus is about the size of a kidney bean and begins to take on the recognizable form of a human being. It’s during the fetal stage that the sex organs begin to differentiate. At about 16 weeks, the fetus is approximately 4.5 inches long. Fingers and toes are fully developed, and fingerprints are visible. By the time the fetus reaches the sixth month of development (24 weeks), it weighs up to 1.4 pounds. Hearing has developed, so the fetus can respond to sounds. The internal organs, such as the lungs, heart, stomach, and intestines, have formed enough that a fetus born prematurely at this point has a chance to survive outside of the womb. Throughout the fetal stage the brain continues to grow and develop, nearly doubling in size from weeks 16 to 28. Around 36 weeks, the fetus is almost ready for birth. It weighs about 6 pounds and is about 18.5 inches long, and by week 37 all of the fetus’s organ systems are developed enough that it could survive outside the uterus without many of the risks associated with premature birth. The fetus continues to gain weight and grow in length until approximately 40 weeks. By then, the fetus has very little room to move around and birth becomes imminent. The progression through the stages is shown in Figure 4.8.
Reproductive Development and Sex Assignment
The first step in differentiation of the reproductive organs happens with a sexless collection of cells at an area called the germinal ridge. In mammals, the main determinant of the pathway the germinal ridge follows is the SRY gene on the Y chromosome. This gene leads to the growth and specialization of cells in the inner portion of the germinal ridge, which eventually become the testes. In the absence of this gene, as in XX individuals, the outer part of the germinal ridge develops into ovaries. Both the testes and ovaries are gonads, reproductive organs that contain reproductive hormones and gametes (sperm or eggs). In most XY individuals, high levels of fetal androgens, like testosterone, released from the testes promote development of the external genitals into a penis. In the absence of testosterone, as in most XX individuals, this same tissue becomes a vagina. The practice of sexing newborn infants in this way has historically led misclassification of intersex people. Therefore, the terms assigned female at birth (AFAB) and assigned male at birth (AMAB) describe biological sex more accurately than female and male, since it includes intersex individuals. This terminology is preferred by many members of transgender, intersex and non-binary communities since it acknowledges an individual’s medical history and allows a distinction between biological sex and gender identity.
DIG DEEPER
Understanding Gender
Gender refers to the way in which one perceives themselves in the historical context of sex and/or gender categories. Gender is largely socially constructed, however, it the form it takes is shaped and influenced by biological sex (American Psychological Association, 2015). So, what does it mean to be a boy or a man? What does it mean to be a girl or a woman?
First let’s start with the basics. “Boy/man”, and “girl/woman” are indeed gender categories that most people identify with. Historically, the categories have been tied to the perceived biological sex of the individual, with “boy/man” correlating to biological males and
“girl/woman” correlating to biological females. A person is “cisgender” when their gender identity matches their assigned sex (i.e., identifies as a woman and was assigned female at birth). A person is “transgender” when their gender identity does not match their assigned sex. (American Psychological Association, 2015). A person is “non-binary” when they don’t identify as either a “boy/man” or “girl/woman”. Non-binary people may or may not also identify as transgender, this will vary from person to person.
In many cultures, gender categories are constructed with the presumption people’s gender identity maps easily onto their (assumed) biological sex. However, there is a lot more to being a man or woman then whether a person has a penis or a vagina and breasts. For instance, masculinity and femininity play a huge role in many people’s conception of their own gender. For most of history, society has been organized by a binary system, male or female, starting with birth certificates. At the moment of birth, every infant is labelled either male or female by a medical authority, and this is usually registered with the government (Preves, 2002). From here, parents and other adults begin to place expectations on who the infant will be as they grow, for instance, what kind of toys they will like or their favorite colour. Because adults start treating the child as a person with gender based on the biological sex before the child has developed their own sense of gender identity, the infant’s own sense of gender reacts and responds to these expectations. Masculinity and femininity is the expression of these reactions and responses. The decision to shave facial hair or not could be considered an expression of masculinity. The decision to wear make-up or not could be considered an expression of femininity. It is not that choosing to wear make-up, or grow out one’s beard makes one more masculine or feminine, so much as the choice is an expression of how one relates to these categories on their own terms. Many women wear make-up, many choose not to. Many men can’t help but grow out long beards, many simply can’t grow one at all (Schippers, 2007).
It would be wrong to suggest that biological sex doesn’t have any influence over gender. Our minds, thoughts, feelings and identities are ultimately generated by the brain and body. For instance, testosterone is a hormone responsible for behaviors and traits associated with social domination and certain types of aggression, such as risk-assessment, initiative and task performance (Goudriaan et al., 2010; Platje et al., 2015; Welling et al., 2016). For many species, biological males experience an increase in testosterone production during puberty, often leading to an increase in muscle mass and body hair and reduction in body fat. Despite popular conception however, this doesn’t make testosterone the “boy/male” hormone since both males and females have measurable levels of testosterone. While it is true that males produce more testosterone, it’s inaccurate to say that testosterone plays no role in female physiology, meaning that testosterone is part of what shapes girls too. Secondly, it’s entirely possible that a cisgender boy may go through puberty and not display any increase in the behaviors associated with testosterone at any point in his life. This doesn’t mean this boy has any less testosterone in his system than his peers (Booth et al., 2006). And even if that were the case, that wouldn’t somehow invalidate the boy’s identity as a “boy” experiencing a “boy’s puberty.
Intersex Conditions
Chromosomal, gonadal, and genital sex most commonly follow either a route to a male reproductive system which donates X and Y gametes via sperm or an XX female system that provides an environment for conception and growth of a fertilized egg. However genetic sex and gonadal sex do not always follow this typical pattern, for example there are XY individuals with vaginas. The external genitals derive from the same tissue so they commonly develop along a continuum with male-typical at one end and female-typical at the other, though some individuals are born with genitals that fall somewhere in the middle of this range. The term intersex refers to individuals who have characteristics that do not fit typical male and female categories. Intersex is an umbrella term to describe many variations, which are sometimes referred to as disorders of sexual development. Since intersex conditions are not harmful to health and usually only affect reproduction, the term disorder to describe these individuals is not accurate.
Chromosomes and gonads are not easy to see, so often the appearance of the external genitals is used to determine sex at birth. However, as mentioned above, this practice has historically led to the misclassification of intersex people. In fact, this can have a number of consequences for the person in question, including a misunderstanding of their own bodies health, and difficulties navigating the medical system. Rates of intersexuality within the human population are difficult to ascertain, especially considering the history of unethical medical intervention on intersex infants. There have been unfortunately many cases of doctors performing unnecessary corrective surgery in order to make the genitals of an intersex infant more “normal”. Occasionally, the parents of the infant may not have been informed of the condition or procedure, nor given their consent. While this is justified as being done to provide the infant with a more normal life, most intersex advocacy groups are strongly opposed to this practice. Often a person has no reason to suspect they are intersex until they reach puberty and, in some cases, it’s only discovered after the death of the individual.
LINK TO LEARNING
For more information on intersex conditions, check out the FAQ for interACT, an advocacy group for intersex youth: https://interactadvocates.org/faq/
Prenatal Influences
The placenta is a structure that develops during pregnancy and provides nourishment and oxygen to the fetus. Almost everything the pregnant parent ingests, including food and medication, travels through the placenta to the fetus, hence the phrase “eating for two.” In fact, the parental environment can have long-term effects on the developing fetus. A teratogen is any environmental agent—biological, chemical, or physical—that causes damage to the developing embryo or fetus. Most teratogens have their greatest impact during early pregnancy. Take for example, lead, which can cause lead poisoning if the pregnant parent becomes exposed from sources like paint or soil. Since the ban on leaded gasoline in the early 90’s, levels in children has declined dramatically, yet childhood lead poisoning remains a global health concern. Research shows that even extremely low levels of lead exposure can still have negative effects, including cognitive impairments (Koller et al., 2004). In the United States alone, deaths related to lead poising are comparable to those caused by smoking tobacco, around 412,000 a year (O’Connor et al., 2020).
Many recreational drugs, like alcohol and tobacco are considered teratogens because they can cross the placenta and negatively affect the fetus. Other teratogens include exposure to radiation and viruses such as HIV, herpes, and rubella (German measles). Additionally, people who experience high stress during pregnancy are more likely to have children with enhanced responses to stress (Leung et al., 2010).
TRICKY TOPIC: PRENATAL DEVELOPMENT
If the video above does not load, click here: https://youtu.be/vN2NRvyQ6Dc
For a full transcript of this video, click here
Infancy Through Childhood
The average newborn weighs approximately 7.5 pounds. Although small, a newborn is not completely helpless because their reflexes and sensory capacities help them interact with the environment from the moment of birth. All healthy babies are born with newborn reflexes: inborn automatic responses to specific forms of stimulation. Reflexes help the newborn survive until they’re capable of more complex behaviours—these reflexes are crucial to survival. They are present in babies whose brains are developing normally and usually disappear around 4–5 months old. Let’s take a look at some of these newborn reflexes.
The rooting reflex is the newborn’s response to anything that touches their cheek: When you stroke a baby’s cheek, they naturally turn their head in that direction and begin to suck. The sucking reflex is the automatic, unlearned, sucking motions that infants do with their mouths. You can observe the grasping reflex if you put your finger into a newborn’s hand, they automatically grasp anything that touches their palms. The Moro reflex is the newborn’s response when a baby feels like they are falling. The baby spreads their arms, pulls them back in, and then (usually) cries. How do you think these reflexes promote survival in the first months of life?
LINK TO LEARNING
What can young infants see, hear, and smell? Newborn infants’ sensory abilities are significant, but their senses are not yet fully developed. Many of a newborn’s innate preferences facilitate interaction with caregivers and other humans. Although vision is their least developed sense, newborns already show a preference for faces. Babies who are just a few days old also prefer human voices, they will listen to voices longer than sounds that do not involve speech (Vouloumanos & Werker, 2004), and they seem to prefer the voice of the parent who was pregnant over a stranger’s voice (Mills & Melhuish, 1974). In an interesting experiment, 3-week-old babies were given pacifiers that played a recording of the pregnant parent’s voice and of a stranger’s voice. When the infants heard their parent’s voice, they sucked more strongly at the pacifier (Mills & Melhuish, 1974). Newborns also have a strong sense of smell. For instance, newborn babies can distinguish the smell of the parent who was pregnant from that of others. In a study by MacFarlane (1978), 1-week-old babies who were being breastfed were placed between two gauze pads. One gauze pad was from the bra of a nursing parent who was a stranger, and the other gauze pad was from the bra of the infant’s own nursing parent. More than two-thirds of the week-old babies turned toward the gauze pad with their own nursing parent’s scent.
Physical Development
During infancy, toddlerhood, and early childhood, the body’s physical development is rapid. On average, newborns weigh between 5 and 10 pounds. By 2 years old, this weight will have quadrupled, with most 2 year olds weighing between 20 and 40 pounds (WHO Multicentre Growth Reference Study Group, 2006). Growth slows between 4 and 6 years old. During this time children gain 5–7 pounds and grow about 2–3 inches per year.
There are two important patterns of development: cephalocaudal and proximodistal. Cephalocaudal development refers to the pattern of growth from the head down, also referred to as development from head to toe. Proximodistal development is the tendency for growth to start in the centre of the body and move outwards to the extremities. This is reflected in the development of more general motor skills of the limbs close to the torso before development of fine motor skills in the fingers and toes.
The nervous system continues to grow and develop after birth; each neural pathway forms thousands of new connections during infancy and toddlerhood. This period of rapid neural growth is called blooming. The blooming period of neural growth is then followed by a period of pruning, where neural connections are reduced. It is thought that pruning allows the brain to function more efficiently, allowing for mastery of more complex skills (Hutchinson, 2011). Blooming occurs during the first few years of life, and pruning continues through childhood and into adolescence in various areas of the brain.
The size of our brains increases rapidly. For example, the brain of a 2-year-old is 55% of its adult size, and by 6 years old the brain is about 90% of its adult size (Tanner, 1978). During early childhood (ages 3–6), the frontal lobes grow rapidly. The frontal lobes are associated with planning, reasoning, memory, and impulse control. Therefore, by the time children reach school age, they are developmentally capable of controlling their attention and behaviour. Through the elementary school years, the frontal, temporal, occipital, and parietal lobes all grow in size. The brain growth spurts experienced in childhood tend to follow Piaget’s sequence of cognitive development, so that significant changes in neural functioning are associated with cognitive advances (Kolb & Whishaw, 2009; Overman et al., 1992).
Motor development occurs in an orderly sequence as infants move from reflexive reactions (e.g., sucking and rooting) to more advanced motor functioning. Motor skills refer to our ability to move our bodies and manipulate objects. Fine motor skills focus on the muscles in our fingers, toes, and eyes, and enable coordination of small actions (e.g., grasping a toy, writing with a pencil, and using a spoon). Gross motor skills focus on large muscle groups that control our arms and legs and involve larger movements (e.g., balancing, running, and jumping).
As motor skills develop, there are certain developmental milestones that young children typically achieve at certain age ranges (Table 4.4) An example of a developmental milestone is sitting. On average, most babies sit alone at 7 months old. Sitting involves both coordination and muscle strength, and 90% of babies achieve this milestone between 5 and 9 months old. In another example, babies on average are able to hold up their head at 6 weeks old, and 90% of babies achieve this between 3 weeks and 4 months old. If a child is displaying delays on several milestones, that could be reason for concern since some developmental delays can be identified and addressed through early intervention.
| Table 4.4 Developmental Milestones, Ages 2–5 Years | ||||
|---|---|---|---|---|
| Age (years) | Physical | Personal/Social | Language | Cognitive |
| 2 | Kicks a ball; walks up and down stairs | Plays alongside other children; copies adults | Points to objects when named; puts 2–4 words together in a sentence | Sorts shapes and colours; follows 2-step instructions |
| 3 | Climbs and runs; pedals tricycle | Takes turns; expresses many emotions; dresses self | Names familiar things; uses pronouns | Plays make believe; works toys with parts (levers, handles) |
| 4 | Catches balls; uses scissors | Prefers social play to solo play; knows likes and interests | Knows songs and rhymes by memory | Names colours and numbers; begins writing letters |
| 5 | Hops and swings; uses fork and spoon | Distinguishes real from pretend; likes to please friends | Speaks clearly; uses full sentences | Counts to 10 or higher; prints some letters and copies basic shapes |
In addition to rapid physical growth, young children also exhibit significant development of their cognitive abilities. Piaget thought that children’s ability to understand objects—such as learning that a rattle makes a noise when shaken—was a cognitive skill that develops slowly as a child matures and interacts with the environment. Today, developmental psychologists think Piaget was incorrect. Researchers have found that even very young children understand physical properties of objects long before they have direct experience with those objects (Baillargeon, 1987; Baillargeon et al., 2011). For example, children as young as 3 months old demonstrated knowledge of the properties of objects that they had only viewed and did not have prior experience with them. In one study, 3-month-old infants were shown a truck rolling down a track and behind a screen. The box, which appeared solid but was actually hollow, was placed next to the track. The truck rolled past the box as would be expected. Then the box was placed on the track to block the path of the truck. When the truck was rolled down the track this time, it continued unimpeded. The infants spent significantly more time looking at this impossible event (Figure 4.11). Baillargeon (1987) concluded that they knew solid objects cannot pass through each other. Baillargeon’s findings suggest that very young children have an understanding of objects and how they work, which Piaget (1954) would have said is beyond their cognitive abilities due to their limited experiences in the world.
Like physical milestones, there are also cognitive milestones children typically reach at certain ages. For example, infants shake their head “no” around 6–9 months, and they respond to verbal requests to do things like “wave bye-bye” or “blow a kiss” around 9–12 months. Remember Piaget’s ideas about object permanence? We can expect children to grasp the concept that objects continue to exist even when they are not in sight by around 8 months old. Because toddlers (i.e., 12–24 months old) have mastered object permanence, they enjoy games like hide and seek, and they realize that when someone leaves the room they will come back (Loop, 2013). Toddlers also point to pictures in books and look in appropriate places when you ask them to find objects.
Preschool-age children (i.e., 3–5 years old) also make steady progress in cognitive development. Not only can they count, name colours, and tell you their name and age, but they can also make some decisions on their own, such as choosing an outfit to wear. Preschool-age children understand basic time concepts and sequencing (e.g., before and after), and they can predict what will happen next in a story. They also begin to enjoy the use of humour in stories. Because they can think symbolically, they enjoy pretend play and inventing elaborate characters and scenarios. One of the most common examples of their cognitive growth is their blossoming curiosity. Preschool-age children love to ask “Why?”
An important cognitive change occurs in children this age. Recall that Piaget described 2–3 year olds as egocentric, meaning that they do not have an awareness of others’ points of view. Between 3 and 5 years old, children come to understand that people have thoughts, feelings, and beliefs that are different from their own. This is known as theory-of-mind (TOM). Children can use this skill to tease others, persuade their parents to purchase a candy bar, or understand why a sibling might be angry. When children develop TOM, they can recognize that others have false beliefs (Callaghan et al., 2005; Dennett, 1987).
LINK TO LEARNING
Cognitive skills continue to expand in middle and late childhood (6–11 years old). Thought processes become more logical and organized when dealing with concrete information (Figure 4.12). Children at this age understand concepts such as the past, present, and future, giving them the ability to plan and work toward goals. Additionally, they can process complex ideas such as addition and subtraction and cause-and-effect relationships.
One well-researched aspect of cognitive development is language acquisition. The order in which children learn language structures is consistent across children and cultures (Hatch, 1983). Starting before birth, babies begin to develop language and communication skills. At birth, babies apparently recognize the voice of their birth parent, and can discriminate between the language(s) spoken by their birth parent and foreign languages, and they show preferences for faces that are moving in synchrony with audible language (Blossom & Morgan, 2006; Pickens, 1994; Spelke & Cortelyou, 1981).
Children communicate information through gesturing long before they speak, and there is some evidence that gesture usage predicts subsequent language development (Iverson & Goldin-Meadow, 2005). In terms of producing spoken language, babies begin to coo almost immediately. Cooing is a one-syllable combination of a consonant and a vowel sound (e.g., coo or ba). Interestingly, babies replicate sounds from their own languages. A baby whose parents speak French will coo in a different tone than a baby whose parents speak Spanish or Urdu. After cooing, the baby starts to babble. Babbling begins with repeating a syllable, such as ma-ma, da-da, or ba-ba. When a baby is about 12 months old, we expect them to say their first word for meaning, and to start combining words for meaning at about 18 months.
At about 2 years old, a toddler uses between 50 and 200 words; by 3 years old they have a vocabulary of up to 1,000 words and can speak in sentences. During the early childhood years, children’s vocabulary increases at a rapid pace. This is sometimes referred to as the “vocabulary spurt” and has been claimed to involve an expansion in vocabulary at a rate of 10–20 new words per week. Recent research may indicate that while some children experience these spurts, it is far from universal (as discussed in Ganger & Brent, 2004). It has been estimated that, 5 year olds understand about 6,000 words, speak 2,000 words, and can define words and question their meanings. They can rhyme and name the days of the week. Seven year olds speak fluently and use slang and clichés (Stork & Widdowson, 1974).
What accounts for such dramatic language learning by children? Behaviorist B. F. Skinner thought that we learn language in response to reinforcement or feedback, such as through parental approval or simply by being understood. For example, when a two-year-old child asks for juice, they might say, “me juice,” to which their parent might respond by giving them a cup of apple juice. Noam Chomsky (1957) criticized Skinner’s theory and proposed that we are all born with an innate capacity to learn language. Chomsky called this mechanism a language acquisition device (LAD). Researchers now believe that language acquisition is partially inborn and partially learned through our interactions with our linguistic environment (Gleitman & Newport, 1995; Stork & Widdowson, 1974).
Attachment
Psychosocial development occurs as children form relationships, interact with others, and understand and manage their feelings. In social and emotional development, forming healthy attachments is very important and is the major social milestone of infancy. Attachment is a long-standing connection or bond with others and is often used to describe the emotional bond between child and caregiver. Attachment is more easily established during the early years of a child’s life and is therefore thought to be reflective of a sensitive period. Developmental psychologists are interested in how infants reach this milestone. They ask such questions as: How do parent and infant attachment bonds form? How does neglect affect these bonds? What accounts for children’s attachment differences?
Researchers Harry Harlow, John Bowlby, and Mary Ainsworth conducted studies designed to answer these questions. In the 1950s, Harlow conducted a series of experiments on monkeys. He separated newborn monkeys from their mothers. Each monkey was presented with two surrogate mothers. One surrogate monkey was made out of wire mesh, and dispensed milk. The other monkey was softer and made from cloth: This monkey did not dispense milk. Research shows that the monkeys preferred the soft, cuddly cloth monkey, even though it did not provide any nourishment. The baby monkeys spent their time clinging to the cloth monkey and only went to the wire monkey when they needed to be fed. Prior to this study, the medical and scientific communities generally thought that babies become attached to the people who provide their nourishment. However, Harlow (1958) concluded that there was more to the birth parent-child bond than nourishment. Feelings of comfort and security are the critical components to parental-infant bonding, which leads to healthy psychosocial development.
LINK TO LEARNING
Building on the work of Harlow and others, John Bowlby developed the concept of attachment theory. He defined attachment as the affectional bond that an infant forms with the parent who birthed them (Bowlby, 1969). An infant must form this bond with a primary caregiver in order to have normal social and emotional development. In addition, Bowlby proposed that this attachment bond is very powerful and continues throughout life. He used the concept of secure base to define a healthy attachment between parent and child (1988). A secure base is a parental presence that gives the child a sense of safety as he explores his surroundings. Bowlby said that two things are needed for a healthy attachment: The caregiver must be responsive to the child’s physical, social, and emotional needs; and the caregiver and child must engage in mutually enjoyable interactions (Bowlby, 1969) (Figure 4.13).
While Bowlby thought attachment was an all-or-nothing process, Mary Ainsworth’s (1970) research showed otherwise. Ainsworth wanted to know if children differ in the ways they bond, and if so, why. To find the answers, she used the Strange Situation procedure to study attachment between parents and their infants (1970). In the Strange Situation, the primary caregiver and child (age 12-18 months) are placed in a room together. There are toys in the room, and the caregiver and child spend some time alone in the room. After the child has had time to explore their surroundings, a stranger enters the room. The caregiver then leaves the baby with the stranger. After a few minutes, the caregiver returns to comfort their child.
Based on how the infants/toddlers responded to the separation and reunion, Ainsworth identified three types of parent-child attachments: secure, avoidant, and resistant (Ainsworth & Bell, 1970). A fourth style, known as disorganized attachment, was later described (Main & Solomon, 1990). The most common type of attachment is called secure attachment (Figure 4.14). In this type of attachment, the toddler prefers their parent over a stranger. The attachment figure is used as a secure base to explore the environment and is sought out in times of stress. Securely attached children were distressed when their caregivers left the room in the Strange Situation experiment, but when their caregivers returned, the securely attached children were happy to see them. Securely attached children have caregivers who are sensitive and responsive to their needs.
With avoidant attachment, the child is unresponsive to the parent, does not use the parent as a secure base, and does not appear to care if the parent leaves. The toddler reacts to the parent the same way they react to a stranger. When the parent does return, the child is slow to show a positive reaction. Ainsworth theorized that these children were most likely to have a caregiver who was inattentive to their needs (Ainsworth et al., 1978).
In cases of resistant attachment, children tend to show clingy behaviour, but then they reject the attachment figure’s attempts to interact with them (Ainsworth & Bell, 1970). These children do not explore the toys in the room, as they are too fearful. During separation in the Strange Situation, they became extremely disturbed and angry with the parent. When the parent returns, the children are difficult to comfort. Resistant attachment is the result of the caregivers’ inconsistent level of response to their child.
Finally, children with disorganized attachment behaved oddly in the Strange Situation. They freeze, run around the room in an erratic manner, or try to run away when the caregiver returns (Main & Solomon, 1990). This type of attachment is seen most often in kids who have been abused. Research has shown that abuse disrupts a child’s ability to regulate their emotions.
While Ainsworth’s research has found support in subsequent studies, it has also met criticism. Some researchers have pointed out that a child’s temperament may have a strong influence on attachment (Gervai, 2009; Harris, 2009), and others have noted that attachment varies from culture to culture, a factor not accounted for in Ainsworth’s research (Rothbaum et al., 2000; van Ijzendoorn & Sagi-Schwartz, 2008).
LINK TO LEARNING
Parenting Styles
While the likes of Harlow, Bowlby, and Ainsworth were studying the development of attachment between an infant and their caregiver, in her seminal work, University of California Berkley’s Diana Baumrind took another position. Baumrind wanted to better understand parent characteristics that contributed to development. Baumrind conducted interviews and observations of parents with their preschoolers (Baumrind, 1971) and found two key characteristic behaviours to have an impact on development: parental demands and parental responsiveness (Baumrind, 1991). Combining the two, Diana Baumrind identified four parenting styles along with child outcomes (Table 4.5).
| Table 4.5 Parenting Styles | ||
| Parental Style | Parental Behaviour | Associated Childhood Outcomes |
| Authoritative | Warm, sensitive to their child’s needs, nurturing, makes reasonable demands, and encourages autonomy | High self-esteem, cooperative, self-control, and social maturity |
| Authoritarian | Cold, rejecting, makes coercive demands, and frequent criticism | Low self-esteem, anxious, unhappy, displays anger and aggressive tendencies |
| Permissive | Warm, accepting, over indulgent but inattentive | Impulsive, disobedient, dependent, and low initiative |
| Uninvolved | Emotionally detached, depressed, little time or energy for their child | Anxious, poor communication skills, and anti-social behaviours |
| Adapted from Ogden et al. (2022) | ||
The sample used in Baumrind’s observations consisted primarily of white, middle-class preschool children and their parents, prompting an important question: How well does Baumrind’s theory apply outside of white, middle-class populations in the United States? Cross-cultural research on parenting styles continue to support Baumrind’s notion of four parenting styles. However, research on Asian populations has revealed the high-demand, low-responsiveness often associated with authoritarian parenting styles to have fewer negative outcomes on children and has even been found to benefit academic performance during adolescence (Chen et al. 2014; Way et al. 2013).
Self-Concept
Just as attachment is the main psychosocial milestone of infancy, the primary psychosocial milestone of childhood is the development of a positive sense of self. How does self-awareness develop? If you place a baby in front of a mirror, they will reach out to touch their image, thinking it is another baby. However, by about 18 months a toddler will recognize that the person in the mirror is them. How do we know this? In a well-known experiment, a researcher placed a red dot of paint on children’s noses before putting them in front of a mirror (Amsterdam, 1972). Commonly known as the mirror test, this behaviour is demonstrated by humans and a few other species and is considered evidence of self-recognition (Archer, 1992). At 18 months old they would touch their own noses when they saw the paint, surprised to see a spot on their faces. By 24–36 months old children can name and/or point to themselves in pictures, clearly indicating self-recognition.
Children from 2–4 years old display a great increase in social behaviour once they have established a self-concept. They enjoy playing with other children, but they have difficulty sharing their possessions. Also, through play children explore and come to explore gender roles (Chick et al., 2002). By 4 years old, children can cooperate with other children, share when asked, and separate from parents with little anxiety. Children at this age also exhibit autonomy, initiate tasks, and carry out plans. Success in these areas contributes to a positive sense of self. Once children reach 6 years old, they can identify themselves in terms of group memberships: “I’m a first grader!” School-age children compare themselves to their peers and discover that they are competent in some areas and less so in others (recall Erikson’s task of industry versus inferiority). At this age, children recognize their own personality traits as well as some other traits they would like to have. For example, 10-year-old Alix says, “I’m kind of shy. I wish I could be more talkative like my friend Ro.”
Development of a positive self-concept is important to healthy development. Children with a positive self-concept tend to be more confident, do better in school, act more independently, and are more willing to try new activities (Ferrer & Fugate, 2003; Maccoby, 1980). Formation of a positive self-concept begins in Erikson’s toddlerhood stage, when children establish autonomy and become confident in their abilities. Development of self-concept continues in elementary school, when children compare themselves to others. When the comparison is favourable, children feel a sense of competence and are motivated to work harder and accomplish more. Self-concept is re-evaluated in Erikson’s adolescence stage, as teens form an identity. They internalize the messages they have received regarding their strengths and weaknesses, keeping some messages and rejecting others. Adolescents who have achieved identity formation are capable of contributing positively to society (Erikson, 1968).
Children develop a personal sense of play style at as young as the second year to life. It’s at this stage we see children start to make choices of individuation, such as toy preference. Toy preference is one of the earliest places we begin to see children develop a sense of gender identity, one study showed gender-based toy preferences at as young as 12-months old (Servin et al., 1999). One might expect that children would show a preferential bias towards toys assigned to the same sex-category as the biological sex of the child, with AFAB children showing a higher preference for “girls’ toys” and AMAB children showing a higher preference for “boys’ toys”. However, the full story is more complex. Parents and authority figures begin instilling children with gender norms based on their own cultural expectations of gender from the moment the child is born. (van de Beek et al., 2006). Because of this, it is possible that children’s expressions of self may be influenced by the expectation that there is a correct way for them to perform self-hood. It also worth keeping in mind that many studies looking at expressions of gender mistakenly use a circular definition in the construction of their categories. A circular definition is a definition that uses one or more of the terms being defined as part of its definition. For instance, it would be circular to claim that violent video game cause teenagers to be violent because violent teenagers play violent video games.
Take for instance a study which attempted to measure the rate at which infants preferred toys assigned to the same gender category assigned to the infant (Alexander et al, 2009). To do this, they tracked rates at which infants visually fixated on one of two toys; a doll (the “girls’ toy”) or a truck (the “boys’ toy”) and compared the amount of time AFAB and AMAB children spent fixated on each toy. The published study claims to have found notable discrepancies in gender-based toy preference. However, there are two major issues. First, the study uses a circular definition in constructing its toy categories. The researchers designated the doll a “girls’ toy” as it was the toy preferred by girls based on the presumption that girls prefer them. The second problem with this study is that their results do not support their claim. Based on average visual fixating on each object, AFAB infants preferred the doll to the truck. AFAB infants spent approximately the same amount of time fixated on the truck as AMAB infants, and AMAB infants actually spent slightly longer looking at the doll than the truck (though this difference was quite small). This underscores the importance of critically evaluating published scientific studies to so as to not mistakenly believe false or misinterpreted conclusions.
So, what can we conclude about children’s early toy preferences and play style? Generally, there are two perspectives on childhood development, one based in the social environment of the child, and one based more in biology. The social environment perspective posits that children’s preferences are influenced by parents and authority figures (such as teachers) who can reinforce or discourage a child’s preferences. The biological perspective claims that children’s preferences are influenced by gonadal hormones, like testosterone (Servin et al., 1999), which is associated with preference for stereotypically masculine toys and physically active “rough and tumble” play (van de Beek et al., 2006). Both the social environment and the presence of hormones are associated with children’s toy preferences, play-style, and self-concept (Chick et al, 2002; Servin et al., 1999).
EVERYDAY CONNECTION
The Importance of Play and Recess
According to the American Academy of Pediatrics (2007), unstructured play is an integral part of a child’s development. It builds creativity, problem solving skills, and social relationships. Play also allows children to develop a theory-of-mind as they imaginatively take on the perspective of others.
Outdoor play allows children the opportunity to directly experience and sense the world around them. While doing so, they may collect objects that they come across and develop lifelong interests and hobbies. They also benefit from increased exercise and engaging in outdoor play can actually increase how much they enjoy physical activity. This helps support the development of a healthy heart and brain. Research suggests that today’s children are engaging in less and less outdoor play (Clements, 2004). While it is true that easier access to calorie-dense food has led to an increase in levels of childhood obesity, this alone does not explain the decrease in physical activity. There are actually a number of factors that may contribute to this decrease in physical activity. Easier access to calorie-dense foods have contributed to increased levels of childhood obesity. It has also become more difficult for children to both access the space required for physical activity and feel safe doing so. Due to parental concerns about things like road safety and stranger danger, children these days have low levels of independent mobility (ie. freedom to travel outdoors without adult supervision). This means that children frequently lack the opportunity to play outdoors. Additionally, factors such as playground overcrowding and the presence of teenagers/older children has been shown to decrease physical activity in children. Play spaces designed to encourage structured activities like team sports may not appeal to all children, many of whom are shown to be more physically active when engaged in activities like creating things or using their imaginations. It has also been shown that children who cross perceived gender norms are likely to be the targets of bullying and/or disapproval from their peers and elders. Due to the gender stereotypes associated with different forms of physical activity, it seems likely that some children may choose to not engage in a physical activity to avoid harassment (inversely, some may choose to participate in an activity solely to avoid the same harassment) (Reimers et al., 2018).
Despite the adverse consequences associated with reduced play, some children are over scheduled and have little free time to engage in unstructured play. In addition, some schools have taken away recess time for children in a push for students to do better on standardized tests, and many schools commonly use loss of recess as a form of punishment. Do you agree with these practices? Why or why not?
Adolescence
Adolescence is a socially constructed concept. In pre-industrial society, children were considered adults when they reached physical maturity, but today we have an extended time between childhood and adulthood called adolescence. Adolescence is the period of development that begins at puberty and ends at emerging adulthood, which is discussed later. In the United States, adolescence is seen as a time to develop independence from parents while remaining connected to them (Figure 4.15). The typical age range of adolescence is from 12 to 18 years, and this stage of development also has some predictable physical, cognitive, and psychosocial milestones.
Because rates of physical development vary so widely among teenagers, puberty can be a source of pride or embarrassment. Early maturing males tend to be stronger, taller, and more athletic than their later maturing peers. They are usually more popular, confident, and independent, but they are also at a greater risk for substance abuse and early sexual activity (Flannery et al., 1993; Kaltiala-Heino et al., 2001). Early maturing females may be teased or overtly admired, which can cause them to feel self-conscious about their developing bodies. These females are at a higher risk for depression, substance abuse, and eating disorders (Ge, Conger, & Elder, 2001; Grabe et al., 1997; Striegel-Moore & Cachelin, 1999). Late blooming males and females (i.e., they develop more slowly than their peers) may feel self-conscious about their lack of physical development. Negative feelings are particularly a problem for late maturing males, who are at a higher risk for depression and conflict with parents (Graber et al., 1997) and more likely to be bullied (Pollack & Shuster, 2000).
The adolescent brain also remains under development. Up until puberty, brain cells continue to bloom in the frontal region. Adolescents engage in increased risk-taking behaviours and emotional outbursts possibly because the frontal lobes of their brains are still developing (Figure 4.16). Recall that this area is responsible for judgment, impulse control, and planning, and it is still maturing into early adulthood (Casey et al., 2005).
LINK TO LEARNING
TRICKY TOPIC: MYELINATION OF THE PREFRONTAL CORTEX
If the video above does not load, click here: https://youtu.be/DHljv1t2_uk
For a full transcript of this video, click here
Cognitive Development
More complex thinking abilities emerge during adolescence. Some researchers suggest this is due to increases in processing speed and efficiency rather than as the result of an increase in mental capacity—in other words, due to improvements in existing skills rather than development of new ones (Bjorkland, 1987; Case, 1985). During adolescence, teenagers move beyond concrete thinking and become capable of abstract thought. Recall that Piaget refers to this stage as formal operational thought. Teen thinking is also characterized by the ability to consider multiple points of view, imagine hypothetical situations, debate ideas and opinions (e.g., politics, religion, and justice), and form new ideas (Figure 4.17). In addition, it’s not uncommon for adolescents to question authority or challenge established societal norms.
Cognitive empathy, also known as theory-of-mind (which we discussed earlier with regard to egocentrism), relates to the ability to take the perspective of others and feel concern for others (Shamay-Tsoory et al., 2005). Cognitive empathy begins to increase in adolescence and is an important component of social problem solving and conflict avoidance.
DIG DEEPER
Developmental Trajectories among Indigenous populations in Canada: The Impact of the Indian Residential School System
Childhood and adolescence are life stages pivotal to someone’s developmental maturation (Cabral & Patel, 2020; Cassidy & Shaver, 2018; White et al., 2017). Experiences such as adversity, loss, trauma, and/or maltreatment have been linked to feelings of anxiety and depression (Hovens et al., 2015; Jurena et al., 2020) as well as issues with attachment in older adult relationships (Cohen et al., 2012; Lo et al., 2017), issues in development (Sege et al., 2017), and other health problems (Asselmann et al., 2018; Nelson et al., 2020; Rojo-Wissar et al., 2021).
Since confederation (1867), the Canadian federal government has continued to forcefully attempt total assimilation of Indigenous peoples into “Euro-Canadian culture and society” (Truth and Reconciliation Commission [TRC], 2015). One of the ways in which the government has attempted to do this was through the Indian Residential School (IRS) system (TRC, 2015). The IRS system in Canada has often been referred to as a series of concentration camps (TRC, 2015) or “boarding schools”used to house Indigenous children. Unlawful and immoral acts perpetuated in the IRSs have been termed “cultural genocide” at the international level (TRC, 2015; United Nations Declaration on the Rights of Indigenous Peoples [UNDRIP], 2007).
Impact on Attachment
From 1876 until the last school closed in 1996, the Canadian federal government physically forced hundreds of thousands of Indigenous children (as young as 4-years-old from their homes and communities, into IRSs (TRC, 2015). Indigenous parents, caregivers and/or family members who showed verbal or physical restraint relative to the police-enforced taking of Indigenous children to IRSs, were often jailed or shot and killed (Bombay et al., 2014ab; Facing History and Ourselves, 2021; TRC, 2015). Once Indigenous children arrived at the schools, many children were stripped, shaved, and had their skin dyed lighter by IRS staff (Smith, n.d.; TRC, 2015). Students were then assigned numbers (used by staff in place of birth names), were separated from their siblings, and told that if they spoke their Indigenous language (the only language most children knew), there would be severe consequences (TRC, 2015). While it is expected that temporary separations from loved ones (e.g., parents) under tense conditions increased the risk of health issues later in life (Räikkönen et al., 2011), extended separations under tense conditions are expected to have increased Survivor risk of depressive symptoms and/or disorders (Bohman et al., 2017; Coffino, 2009) and anxiety symptoms and/or disorders (Bryant et al., 2017; Lähdepuro et al., 2019).
Intergenerational Impacts
Federal, institutional and academic inquiries into the IRS system continue to highlight various atrocities experienced by many IRS Survivors such as spiritual, verbal, emotional, physical and sexual assault, abuse and violence (TRC, 2015). Trauma of this magnitude continues to impact not only the Survivors, but their children, grandchildren, and other relatives (Bombay et al., 2014ab). This phenomenon, known as intergenerational trauma, has direct and indirect impacts on various generations of Indigenous populations (Bombay et al., 2014ab; Lehrner & Yehuda, 2018). For example, Indigenous children of IRS Survivors are more likely to have poor psychological health because of the IRS impacts on their parents’ psychosocial functioning and health (Bombay et al., 2011, 2014ab; 2018; Elias et al., 2012; Kaspar, 2014).
Biopsychosocial Framework
In general, a Biopsychosocial Framework has been characterised by the ways biological, psychological, and social factors can affect an individual and helps health practitioners conceptualize manifestation of particular physical or mental health issues (Karunamuni et al., 2020). With this framework, it is not hard to understand that while many IRSs delivered/had poor curriculum, instruction, staffing, and high levels of racism (Barnes & Josefowitz, 2019; TRC, 2015), many Survivors were academically ill-equipped (e.g., lacked adequate language proficiency; Barnes et al., 2006) and oftentimes extremely poorly prepared for adult employment (Miller, 1996; TRC, 2015). It is expected that the cumulative trauma experienced at the IRSs lead to many Survivors struggling with psychosocial well-being/regulation, connection with other Indigenous socio cultural customs, practices and peoples, and physical and mental health difficulties (Barnes et al., 2019; Miller, 1996; Ogle et al., 2013; TRC, 2015; Vachon et al., 2015).
Cumulative Risk
Cumulative risk can be understood as the number and severity of adversities (e.g., low SES, addict parent or caregiver) experienced in childhood, wherein a greater number and severity of adversities often “adds” to a greater risk of an individual to experience later physical and mental health issues (Boles, 2021; Kwong & Hayes, 2017; Felitti & Anda, 2009; Felitti et al., 1998). Putting this research into context, IRS Survivors who underwent separation from parents, and experienced abuse, racism, and forced immersion in a hostile non-Indigenous culture, were all factors that had a cumulative impact and amplified adverse effects of their adverse experiences at IRS (McQuaid et al., 2017; Richmond et al., 2009). As many Indigenous peoples were directly or indirectly affected by IRSs and colonization, in combination with deficient health resources/geographical isolation, and other ongoing inequities, it is not surprising that many health inequities faced by Indigenous peoples documented 20 years ago, are still faced today (Gracey & King, 2009; RCAP, 1996; TRC, 2015).
Cultural Resilience
While Indigenous peoples in Canada continue to face premeditated colonial assimilation tactics, such as the child welfare crisis or “modern day IRS system” (Ma et al., 2019; McMillan, 2021; Mitchell, 2019), resilience among Indigenous populations in Canada continues to be researched (Bombay et al., 2010, 2011; Paul et al., 2022). To date, various facets of cultural identity among Indigenous populations in Canada have shown to be protective of the negative effects of colonization, such as cultural community belonging (Bombay et al., 2014ab; First Nations Health Authority, 2019; Paul et al., 2022). While Indigenous culture has been suggested to be protective and stabilize and/or heighten various aspects of health and wellbeing (e.g., Paul et al., 2022), continued research is needed to better understand how these cultural facets can be implemented in culturally-appropriate care models for Indigenous populations.
To learn more about Indian Residential Schools, visit: https://www.youtube.com/watch?v=2zuRQmwaREY
