4 Chapter 4: Learning Disabilities
Jennifer Canning; Darean McCormick; Truong Vo; and Conor Barker
In this chapter, you will learn about learning disabilities. First, we introduce the basics of learning disabilities—the different processes learning disabilities affect, who is most likely to have learning disabilities, and how learning disabilities are categorized and diagnosed. We also provide a brief overview of the history of learning disabilities. Once you master the basics, you can read more in-depth about the symptoms corresponding to each subtype of learning disability. This chapter will also explore contributing developmental factors of learning disabilities, as well as currently available interventions. Finally, at the end of this chapter, you will have the chance to test your knowledge of learning disabilities by playing the end of chapter H5P activity!
Learning Objectives
Understand the diagnostic criteria of learning disabilities.
Be familiar with past and present stigmatization of learning disabilities.
Understand assessment and intervention tools for the four categories of learning disabilities.
Describe the main factors contributing to learning disabilities.
Distinguish between the four categories of learning disabilities (reading, writing, mathematics, and non-verbal).
What is a Learning Disability?
Simply put, a learning disability involves difficulty understanding or producing information, typically in at least one of the following areas: reading, writing, or mathematics (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021). Learning disabilities occur in early developmental periods and, on average, affect an estimated 10% of the population, ranging from approximately 3.2% – 15% (American Psychiatric Association, 2013; Grigorenko et al., 2020; Learning Disabilities Association of Canada, 2021). Though no single cause has been determined, recent research suggests that the difficulties experienced by those with learning disabilities may be partially attributed to atypical executive functioning (Crisci et al., 2021; El Wafa et al., 2020; Malekpour & Aghababaei, 2013). Those diagnosed with a learning disability can—and often do—display deficits in executive functions, such as a reduced ability to coordinate fine motor movements, problem solve, encode, recall, express, and actively use information relating to one of the three areas affected by the learning disability (i.e., reading, writing, and mathematics). Additionally, functional and structural differences in the brains of those with learning disabilities have been observed compared to typically developing populations. Unique differences can also be observed across reading, writing, and mathematical subtypes of learning disability (Grigorenko et al., 2020). Hence, a learning disability is considered a neurodevelopmental disorder and is one of the most common forms of disability observed in school-aged children (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
Coping with Learning Disabilities
Despite no “cure” for learning disabilities, early intervention and support can significantly improve academic, occupational, and social performance outcomes. Various interventions are available to reduce stress associated with difficulty in these performance areas (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021). Therefore, despite being a lifelong diagnosis, the outlook for those with learning disabilities is promising. For starters, due to the prevalence of learning disabilities and the push toward inclusive learning environments, teachers nowadays receive more opportunities for training and external support (e.g., school psychologists, learning strategists). These individuals specialize in working alongside students with learning disabilities (Grigorenko et al., 2020; Noyes et al., 2022). Advocacy for more inclusive education has also led to more group work, peer-facilitated learning, and strength-based teaching. Peer-facilitated learning encourages students of similar grade levels and ages to learn new material by teaching each other what they know. Peer-facilitated learning can be quite effective at improving academic and social skills and enhancing positive interactions between children diagnosed with learning disabilities and their peers. Strength-based teaching methods encourage children to compensate for their weaknesses by identifying and utilizing their strengths. Hence, these methods can increase students’ self-efficacy and self-worth, which can be particularly helpful for students with learning disabilities who lack confidence due to their diagnosis (Fuchs et al., 2002). Finally, although uncommon, it is possible to be diagnosed with co-occurring learning disability and giftedness. Giftedness refers to above-average potential for high achievement in tasks requiring cognitive and non-cognitive abilities, such as problem-solving ability and creativity, respectively. It has been found that students who demonstrate both giftedness and some form of learning disability are often highly motivated, exhibit practical coping skills, and demonstrate high levels of perseverance, especially compared to their typically developing, non-gifted peers (Beckmann & Minnaert, 2018).
Diagnostic Criteria
When diagnosing learning disorders, there are often discrepancies between the criteria used by health and medical professionals and the diagnostic guidelines favoured by educators. As the name suggests, the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) is a diagnostic resource developed by the American Psychiatric Association which contains information about common signs and symptoms of various biological, psychological, and social disorders (American Psychiatric Association, 2013). Most psychologists in North America—including many school psychologists—rely on the DSM-V when conducting psychological assessments and making diagnoses. The same tends to be true for medical and health professionals when diagnosing and creating intervention plans for students with learning disabilities.
According to the DSM-V, requirements to meet diagnostic criteria for a learning disability include: a) “symptoms persisting for at least six months, despite the provision of interventions that target those difficulties,” b) affected academic skills are below what is expected for the person’s age and cause significant impairment in academic performance or daily living, c) learning difficulties arise during school ages but may not become apparent until academic demands exceed the individual’s capacity, and d) “the learning difficulties are not better accounted for by intellectual disabilities, uncorrected visual or auditory acuity, other mental or neurological disorders, psychosocial adversity, lack of proficiency in the language of academic instruction, or inadequate educational instruction.” Assessment should only be conducted by qualified clinical professionals (e.g., clinical psychologists, school psychologists, and psychiatrists) (American Psychiatric Association, 2013).
Some school psychologists and educators reference the diagnostic criteria and conceptualization proposed by the Learning Disability Association of Canada (LDAC). The LDAC is a non-profit organization, primarily run by volunteers from all over Canada, consisting of parents, researchers, medical and health professionals, lawyers, educators, and a variety of intervention specialists. LDAC’s purpose is to educate the general public on learning disabilities via the dissemination of research and through opportunities for workshops and collaborative events, as well as to develop and direct individuals with learning disabilities and their families to effective preventions, interventions, and supportive communities (Learning Disabilities Association of Canada, 2021).
Similarities and Differences Between the DSM-V and LDAC
The DSM-V categorizes learning disabilities as neurodevelopmental disorders. As explained previously in this chapter, neurodevelopmental disorders are characterized by the onset of executive functioning deficits early in development, which are thought to have biological bases and can subsequently hinder academic, occupational, recreational, and social performance. The DSM-V clarifies that learning disabilities can be diagnosed in adulthood. However, there must still be evidence of onset in early childhood, as onset later in life would indicate some other disorder. Additionally, learning disabilities are distinct from intellectual disability in that they are characterized by particular impaired abilities rather than comprehensive impairments across multiple ranges of ability, which is observed in intellectual disability (American Psychiatric Association, 2013).
Similar to the DSM-V, LDAC recognizes learning disabilities as neurological disorders. LDAC also emphasizes that learning disabilities should be recognized as distinct from intellectual disability. Interestingly, LDAC provides comparatively more information than the DSM-V regarding the influence of learning disabilities on communication and social behaviours (Learning Disabilities Association of Canada, 2021).
Although there is a significant overlap in information on learning disabilities highlighted in the DSM-V and provided by LDAC, two key differences may explain why educators and medical-health professionals prefer one resource over the other. First, as mentioned above, the DSM-V and LDAC define learning disabilities differently regarding social skills. The DSM-V emphasizes the negative consequences that learning disabilities can have on a child’s academic (i.e., cognitive) abilities. In contrast, LDAC provides more discussion on how learning disabilities can negatively impact relationships and socialization. Perhaps then, some educators and school psychologists prefer the LDAC definition of learning disabilities because it emphasizes the effects that learning disabilities can have on socialization. Social learning is a significant factor in how young children learn and is much easier to observe in the classroom than in a hospital or clinical setting (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
Second, LDAC uses the term learning disability, whereas the DSM-V categorizes learning disabilities as neurodevelopmental disorders and utilizes the term specific learning disorder. Why does this matter? Psychologists are used to using medical terminology such as disorder, but educators are not. Some may find that such terms can be stigmatizing and prefer the term disability, as it has fewer negative connotations. Therefore, given the importance of inclusive education practices, it is possible that educators—and even some school psychologists—are in favour of the information presented by LDAC, as they are advocates for disability terminology rather than the potentially stigmatizing disorder terminology that the DSM-V reinforces (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
History of Learning Disabilities
The following are a few common misconceptions regarding learning disabilities today. We ask that you keep these examples in mind, as information provided throughout the rest of this chapter can be used to disprove them.
- Despite being recognized as a unique disorder, ADHD is often mistaken as a learning disability. It is not. It is true that ADHD and learning disabilities are considered neurodevelopmental disorders and can co-occur, yet they have many salient symptoms and traits (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
- Learning disability and intellectual disability are two mutually exclusive disorders. However, many people incorrectly assume they are the same and use these terms interchangeably. This is false. In reviewing the DSM-V and LDAC diagnostic criteria for specific learning disorder and learning disability, we see that learning disabilities can only be diagnosed if symptoms are not attributable to other disorders, like intellectual disability (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
- Some believe that having a learning disability makes an individual less intelligent. A learning disability does not equate to having a low IQ (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
- People often think that dyslexia is the only type of learning disability. While being the most commonly diagnosed, dyslexia is not the only form of learning disability. Learning disabilities can affect one or more areas of learning, such as reading, writing, and mathematics, and each has unique subtypes (American Psychiatric Association, 2013; Learning Disabilities Association of Canada, 2021).
- Another false belief about learning disabilities is that they naturally improve over time. This is incorrect. Learning disability is a lifelong diagnosis that does not improve without intervention (Learning Disabilities Association of Canada, 2021). Symptoms may present less severely in adults, as adults are less likely to be in academic environments that require reading, writing, and mathematical achievement. Despite this, the learning disability is still present.
- A longstanding misconception is that learning disabilities result from laziness and lack of effort to learn. Therefore, some believe that learning disabilities can be “cured” by studying harder. This is false, as we know that learning disabilities are officially categorized in the DSM-V as neurodevelopmental disorders. This means that learning disabilities are primarily caused by biological and genetic factors (American Psychiatric Association, 2013; Grigorenko et al., 2020; Learning Disabilities Association of Canada, 2021). Additionally, individuals with learning disabilities often have to study harder than their peers and thus should not be labelled lazy.
Figure 1
Common Misconceptions and Facts About Learning Disabilities
|
Misconception |
Fact |
|
ADHD is a type of learning disability. |
ADHD is also a neurodevelopmental disorder, but it is not a type of learning disability. |
|
Learning disability and intellectual disability are the same thing. |
Both are neurodevelopmental disorders, but learning disability and intellectual disability are not the same. |
|
Learning disability = low intelligence |
Learning disabilities are not caused by, and do not result in, low intelligence. |
|
Dyslexia is the only type of learning disability. |
Dyslexia is one of many types of learning disability. |
|
You can naturally “outgrow” a learning disability. |
Learning disability is a lifelong disorder. |
|
Learning disabilities reflect laziness and a lack of motivation to learn. |
“Trying harder” in school will not get rid of a learning disability. |
Note: Made using Microsoft Word. (American Psychiatric Association, 2013; Grigorenko et al., 2020; Learning Disabilities Association of Canada, 2021).
Have you heard others or found yourself engaging in the stereotypes and misconceptions highlighted above? It is clear that individuals with learning disabilities still face stigmatization today; however, the discrimination they faced only a few decades ago was more severe. Present-day prejudice is likely due to a previously poor understanding of learning disabilities, in addition to a lack of support for and the persistent maltreatment of individuals with learning disabilities, all of which we cover in this section. Our discussion begins with past hypotheses of the causes of learning disabilities, followed by a summarization of previous stigmatization and maltreatment resulting from said misconceptions. Finally, we end with a timeline of important events that led to our current understanding of learning disabilities (Thornberry & Olson, 2005).
Previous Categorizations of Learning Disabilities
Individuals with learning disabilities and their families were often ostracized and maltreated by their neighbours, educators, and peers. Practitioners and medical professionals ignored parents seeking help for their children and, in more severe cases, encouraged parents to institutionalize their children (Mitchell, 2006; Thornberry & Olson, 2005). This can partly be explained by the fact that before the 1980s, learning disabilities were not recognized as unique disabilities (American Psychiatric Association, 1968, 1980; Grigorenko, 2016). At this time, individuals with intellectual disabilities were severely maltreated because they were viewed as below others and a threat to society (Thornberry & Olson, 2005). Learning disabilities were often lumped in with intellectual disability. Hence, the same maltreatment also occurred to individuals with more severe presentations of learning disabilities.
Historical Maltreatment
Children with intellectual disability have historically been at increased risk for various types of abuse at home, school, and recreational environments (Thornberry & Olson, 2005). A recent study by Helton et al. (2018) found that even today, young children with learning disabilities are more likely to experience sexual abuse than their non-diagnosed, same-aged peers. Results indicated that the chance of sexual abuse was estimated to be 2.5 greater when a learning disability was present. Authors suggested that historically, the reason children with learning disabilities might be the target of sexual abuse—and other forms of abuse—is due to their reduced social awareness, decreased communication skills, and reliance on adults around them. In other words, abusers may consider them less likely to report abuse and more easily trusting than their peers (Helton et al., 2018).
Frequently prescribing ineffective and sometimes harmful medications were a standard and convenient option for treating those with disabilities. Institutionalization was another solution for disability in the past, and it was often suggested for more severe cases of disability. However, the idea of institutionalization was deceptively proposed to parents as beneficial for both them and their children. For example, parents were persuaded that their lives would be easier if they institutionalized their children, as they could devote less time to caring for them.
Additionally, parents were reassured that professionals in these institutions would deliver better care than what could be provided at home. This was a false promise, as we know that at that time, causes of learning disabilities were less well understood, and there were few empirically-supported interventions. Instead of the support and rehabilitation that children and their parents were promised, institutionalization typically led to abuse, neglect, and overmedication (Helton et al., 2018).
The Evolution of Perspectives on Learning Disabilities
We now explore a timeline of important events, research, and organizations that have positively impacted and moulded how we understand and support learning disabilities today.
1676: Characteristics similar to those of modern learning disabilities were observed in humans dating as far back as 1676. Johannes Schmidt described and documented these traits (Grigorenko et al., 2020).
1950s: Edward Levinson was a Canadian researcher that pioneered empirical research on learning disabilities in Canada (Stegemann, 2016).
1960: In 1960, Edward Levinson helped create the Montréal Children’s Hospital Learning Centre to further increase the opportunity for research on learning disabilities in Canada (Stegemann, 2016).
1962: LDAC was officially founded—primarily due to the parents of individuals with learning disabilities—in Ottawa, Canada, between 1962 and 1963 (Learning Disabilities Association of Canada, 2021; Stegemann, 2016).
1968: The DSM-II was published in 1968. It categorized symptoms of SLDs and ADHD under “mild brain damage.” However, it clarified that these traits were not attributable to below-average intelligence (American Psychiatric Association, 1968; Grigorenko et al., 2020).
1980: The DSM-III was published in 1980. It recognized for the first time that ADHD and academic skill disorders (i.e., a precursor to what we now know as SLDs) are, in fact, distinct disorders (American Psychiatric Association, 1980; Grigorenko et al., 2020).
1981: LDAC first attempted to officially define learning disability in 1981 (Stegemann, 2016).
1994: The DSM-IV was published in 1994. It was the first edition of the DSM to distinguish between three subtypes of SLD (i.e., reading, mathematics, and written expression) (American Psychiatric Association, 1994; Grigorenko et al., 2020).
2013: The DSM-V was published in 2013. It moved away from aptitude-achievement discrepancy criteria for identifying SLDs and suggested symptoms must persist despite receiving adequate education and targeted interventions (American Psychiatric Association, 2013; Grigorenko et al., 2020).
Present: As a result of a profound lack of medical and professional support in the past, the parents of those with learning disabilities remain the most influential advocates for improved access to resources and the advancement of research on learning disabilities (Mitchell, 2006; Stegemann, 2016). As a result, modern interventions are much more specialized and can be tailored to individual strengths and weaknesses, as well as to different subtypes of learning disabilities.
Figure 2
A Visual Timeline of Important Events in the History of Learning Disabilities
Note: Made using Microsoft SmartArt. (American Psychiatric Association, 2013; Grigorenko et al., 2020; Learning Disabilities Association of Canada, 2021; Mitchell, 2006; Stegemann, 2016).
Learning Disabilities in Reading
Learning to read is a foundational skill established in early education, and difficulties developing this skill have serious negative consequences for learners. Reading requires knowledge from the environment and adequate cognitive-linguistic abilities. Cognitive-linguistic abilities include processing spoken language to recognize the sound of words and develop phonemic awareness, visually encoding symbols (e.g., the shapes of letters) that form printed text, and using one’s understanding of language to code, store, and retrieve information for future processing (Vellutino et al., 2004).
Individuals who demonstrate difficulties in reading are diagnosed with learning disabilities (LD) in reading, or as listed in the DSM-V, specific learning disorders (SLD) in reading. Reading problems include difficulties with accurate word reading, reading fluency, and reading comprehension. Learning disabilities in reading can be diagnosed at any age, ranging from elementary-aged youth to adults. In this chapter, our primary focus is on students in their elementary years.
Children diagnosed with learning disabilities in reading have difficulty decoding words, lack phonetic awareness, and trouble with word-level recognition and comprehension (American Psychiatric Association, 2013). As children with LD in reading demonstrate problems with reading individual words and words in context (Gayan & Olson, 2001), the DSM-V and Individuals with Disabilities Education Act (IDEA, 2004) agree that children with learning disabilities in reading have difficulties reading single words and difficulty with reading comprehension.
Learning disabilities in reading are often called dyslexia, a reading disorder associated with difficulties in decoding, phonetic knowledge, and word recognition. However, not all learning disabilities in reading are dyslexia. To support this point, LDAC (2015) includes difficulties in word comprehension in the category of reading disabilities. In this section, we learn about the two levels of learning disabilities in reading: word-level, which is referred to as dyslexia, and text-level, which refers to difficulties in reading comprehension. We also discuss factors that make some students more vulnerable to learning disabilities in reading and examine past and present measures of assessment and intervention.
Dyslexia
One of the most well-known learning disabilities in reading is dyslexia, which is listed as a specific reading disorder in the DSM-V. The International Dyslexia Association (IDA, 2014) defines dyslexia as a neurologically based disorder, which is also accepted and used by the National Institute of Child Health and Human Development (NICHD). Children with dyslexia usually have deficits in phonological awareness, meaning they lack knowledge of the sound structure of language. Children with poor phonological awareness have a limited understanding of how to construct and manipulate sounds and syllables that form words and sentences. Thus, they need help figuring out how printed words sound. Children with dyslexia also display poor phoneme awareness, an underlying structure of phonological awareness that helps individuals read fluently. Low phonemic awareness includes deficits in segmentation (i.e., breaking words down at the letter level, decoding, and rearranging words) (Hulme & Snowling, 2016). Children with dyslexia often have difficulty distinguishing the similarities and differences between letters and words, recognizing familiar words, pronouncing unfamiliar words, and spelling accurately (American Psychiatric Association, 2013).
TED-Ed. (2013). What is dyslexia? – Kelli Sandman-Hurley. [Video].
https://www.youtube.com/watch?v=zafiGBrFkRM
Early Signs and Risk Factors
Figure 3
Early Signs of Word- and Text-level Reading Disabilities
|
Early Signs of Learning Disability in Reading, Word-Level |
Early Signs of Learning Disability in Reading, Text-Level |
|
|
Note: Made using Microsoft Word. (Mayo Clinic, 2022; American Psychiatric Association, 2013).
Children exposed to environmental risk factors may develop learning disabilities in reading. Risk factors include weak cognitive and socioemotional resilience (Haft et al., 2016), lack of parental education, low socioeconomic status, genetics (Gilger et al., 1991), and poor maternal mental health (Carotenuto et al., 2017). These factors can interfere with a child’s ability to develop language and literacy skills by not providing an ideal environment for children to develop reading skills and adapt to their LD in reading. Risk factors can also interfere with children receiving support from others. Since risk factors are modifiable, understanding them can identify children at risk and provide early learning opportunities to help them succeed academically and socially.
Demographics
Previous studies demonstrate that learning disabilities in reading are more common in males than females. However, recent studies on gender differences tend not to show a discrepancy in gender ratios. For learning disabilities in reading at the text-level, the prevalence is estimated to range from 1% – 15% in school-age children (Fletcher et al., 2018). However, learning disabilities in reading at the word-level is the most common type of LD—the worldwide prevalence is approximately 15% – 20% of the population. Similar to LDs in writing and mathematics, the onset of LDs in reading usually occurs during the early elementary school years—a time when children are exposed to academic contexts. At this point, children will need to use their academic reading skills to process and comprehend words in texts.
Cultural & Language Differences
Cultural differences are often under addressed in research on learning disabilities in reading. There is a belief that phonological and alphabetical systems in each language are different. If children grow up in a bilingual family, it is suggested that they have a higher chance of experiencing reading disabilities. Steve et al. (1982) suggested that in the past, Japanese and Chinese people did not have the vocabulary to describe reading disabilities. Therefore, their resources and research on reading disabilities were limited.
Contributing Factors
Neurological
There is evidence of a correlation between the connectivity in the left insula and right cerebellum, and phonological awareness (Ang et al., 2020), which suggests that lesions or functional deficits in these areas affect children’s knowledge of phonological awareness. The ventral, dorsal, and anterior circuits may also be involved in learning disabilities in reading. The ventral circuit is comprised of the left lateral extra-striate, which refers to areas other than the primary visual cortex that are responsive to visual stimuli (Kaufman et al., 2011), and inferior occipital-temporal regions. The ventral circuit children’s ability to recognize familiar words and letters quickly. Poor decoding ability is related to the dysfunction of the dorsal circuit, which includes the left superior temporal and inferior parietal structures. The third circuit is the anterior circuit, which includes the inferior frontal gyrus (Broca’s area). It is involved in children’s ability to comprehend language. Deficits in this area will increase the possibility of having LD in reading at the text-level in children (Pugh et al., 2000; Shaywitz et al., 2006, as cited in Jagger-Rickels et al., 2018).
Despite structural differences in the brains of individuals with genetic traits associated with LD in reading, compared to typically developing samples, individuals with such traits have good reading skills. Therefore, it is not certain that differences in these brain structures lead to LDs in reading. Researchers must investigate the relationships between chemical connections within the brain and neuronal activity to pinpoint the possible cause(s) of learning disabilities in reading (International Dyslexia Association, 2020).
Genetic
Most studies investigating the genetic etiology of LDs in reading are twin studies, and heritability has been strongly supported. Learning disabilities in reading are stable. The heritable traits within the family support stability; genetic factors are responsible for approximately 75% of this stability (Astrom et al., 2007). If parents have difficulties in reading, there is a 60% chance their children will develop dyslexia (Schumacher et al., 2007). On the other hand, Scarborough (1990, as cited in Shaywitz & Shaywitz, 2005) proposed that children whose parents have dyslexia have a 65% chance of having other learning disabilities in reading.
Children with learning disabilities in reading are placed under much pressure from parents, teachers, and peers. Children exposed to excessive stress and pressure develop an adaptive response to stressful stimuli. They are exposed to glucocorticoids which can alter the circulation of cortisol levels and result in HPA axis hyperfunction. This adaptation in stressful situations makes children “careless” to the stress of having learning difficulties (Theodoridou et al., 2021).
Symptoms and Diagnostic Criteria
The DSM-V (2013) indicates that children are diagnosed with significant impairment in reading ability if difficulties in the following areas persist for at least six months: reading words accurately or quickly, reading effortfully, difficulties comprehending text, and difficulties spelling. Additionally, their reading ability is significantly below the standard for their age, measured intelligence, and education. Reading ability must also be considered below average for one’s chronological age.
Assessment Process
Assessment is crucial in identifying and supporting children with LDs, especially early on. Universal screening is an effective method to identify children at risk for LDs. Assessment for LDs in reading includes brief and standardized measurements that score students based on age and grade-specific language skills. Language skills include phonemic awareness, phonics, decoding for pre-elementary and grade one students, and oral reading fluency and reading comprehension for older students (Malcolm, 2022).
Another assessment tool for learning disabilities in reading is the Wechsler Individual Achievement Test (WIAT-III). The WIAT-III measures academic skills in reading, mathematics, and written language (Gregoire & Desoete, 2009). Test results are used to identify areas of strengths and weaknesses. The GORT-5 is a popular test used to measure oral reading fluency and comprehension, which evaluates LDs in reading at the text-level. In addition, the TOWRE-2 can be used to assess students’ ability to pronounce words.
Supports and Interventions
Early intervention is critical to help children with learning disabilities overcome obstacles and prevent long-term social and academic problems. One of the approaches is the Response to Intervention Framework (Stecker et al., 2020), a multi-tiered system that supports students with the increase in academic reading demands as school progresses. Using data from assessments, the framework identifies students’ needs based on their responses to assessment programs. Once the need level increases, interventions get more intensive. There are other programs, such as Peer-Assisted Learning Strategies (PALS), where teachers pair two students to work together. One student in the pair has typical reading skills, while the other needs reading support. The students take on the roles of tutor and tutee, respectively (Institute of Education Sciences, 2007).
Another program designed for small groups is the Empower Reading Program. It has five modules for LDs in reading intervention: decoding, spelling, reading comprehension, and vocabulary, which supports different age groups. This program provides various approaches to teaching students reading skills, methods to support students to become independent readers, and activities to monitor student progress and strengthen students’ confidence (SickKids, 2022). The programs mentioned above can work together in the intervention plan as a multi-tiered approach to support students with different needs in different contexts, such as in class or small groups.
LDAO (2014) The Tiered Approach [Video]
Learning Disabilities in Mathematics
Learning disabilities in mathematics include difficulties in any or all the following areas: learning number sense and other basic numerical concepts, accurately performing basic arithmetic operations, solving math problems, comprehending mathematical concepts, symbols, and vocabulary, applying mathematics to solve problems in daily life, and mastering complex mathematical concepts, equations, and algorithms (Wilson & Swanso, 2001). There are two primary learning disabilities in mathematics: operations and problem-solving. Operations refer to basic arithmetic operations such as addition, subtraction, multiplication, and division. On the other hand, problem-solving is using these operations to solve complex problems, such as fractions, percentiles, and geometry (Fuchs & Fuch, 2002).
To succeed in math, students must be proficient in operations and problem-solving. Operations are the foundation upon which problem-solving is built. To solve a problem, students need to understand the question and break it down into smaller pieces. Then, they must identify and carry out the operation to help them solve the problem. Once they have done this, they can check their work to verify that they arrived at the correct answer. Problem-solving requires a higher level of critical thinking than operations. In addition to being able to understand and carry out operations, students need to think abstractly and see patterns (Fuchs & Fuch, 2002). They also need to be able to approach problems from different angles and use trial and error to find solutions. Both types of disabilities can significantly impact a student’s ability to succeed in mathematics.
Although the cause of mathematical disabilities is not fully understood, research suggests they are neurological and heritable. As such, mathematical disabilities are considered lifelong conditions that cannot be cured. However, with early intervention and specialized instruction, most individuals with mathematical disabilities can learn to develop compensatory strategies and overcome many of their difficulties.
Dyscalculia
Dyscalculia in the DSM-V (2013) is a specific learning disorder in mathematics. It affects individuals’ ability to understand and work with numbers and can cause problems with counting, estimating, mental arithmetic, and calculating (Butterworth et al., 2011). Dyscalculia can impact every area of an individual’s life where mathematical skills are required, including at home, work, and leisure activities. These difficulties can also lead to low self-esteem and a lack of confidence. Table 2 shows early signs in children with a higher risk of developing dyscalculia in the future, considering environmental, genetic, and neurological risk factors.
Figure 4
Early Signs and Risk Factors of Dyscalculia
Note: Made using Microsoft Word. (Gregoire & Desoete, 2009; International Dyslexia Association, 2020; Jordan et al., 2010; LeFevre et al., 2010; Slot et al., 2016).
Ten Braak et al. (2022) posit that as children enter preschool and begin to learn more formal mathematics concepts, early predictors (see Table 2) of mathematics disabilities become more apparent. Poor performance on tasks measuring counting skills, number knowledge, and spatial skills are all associated with later mathematics difficulties. In addition, preschoolers who show a lack of interest in mathematics or who have difficulty completing mathematics tasks are at risk for later mathematics disabilities.
The Centre of Education and Youth. (2020). Introduction to dyscalculia. [Video].
https://www.youtube.com/watch?v=ClW7nw6JGAI
Early Signs and Risk Factors
The signs of learning disabilities in mathematics can be observed in preschool children through their interaction and interest in activities. For instance, children may have difficulty remembering names of numbers, or learning how to count. Entering elementary school, children may have difficulties learning math facts, failing to match the magnitude of a number with that number. Children also have trouble sequencing numbers and conducting simple arithmetic procedures (American Psychiatric Association, 2013).
A study by Barry (2006) suggested that risk factors for learning disabilities in mathematics, such as family background and socio-economic status, have important implications for prevention and intervention efforts. First, it highlights the importance of targeting early intervention programs for children from disadvantaged backgrounds. Second, it suggests that efforts to improve academic achievement for all children should focus on reducing socioeconomic disparities (Barry, 2006). Finally, the literature underscores the need for continued research into the role of family background and socio-economic status in the development of LDs in mathematics. There is also evidence that specific family characteristics are associated with an increased risk for mathematics difficulties. Additionally, children of parents who did not complete high school are more likely to have mathematics difficulties.
However, early signs and risk factors do not always result in the development of a mathematical disability. Many children who struggle with early numeracy skills and working memory become successful math students. Therefore, it is important to provide support and interventions for struggling students as early as possible.
Demographics
LD in mathematics can occur at any age, but it is most often diagnosed in children between the ages of 5 and 7 (Devine et al., 2013). Estimates of the prevalence of LDs in mathematics vary widely, but it is generally agreed that the condition affects approximately 5-7% of the population. Similar to other LDs, the age of onset for learning disabilities in mathematics is during childhood or adolescence, when children are exposed to the academic context and need to solve mathematics problems.
While learning disabilities in mathematics rates seem to be even in arithmetic between genders, there is a difference when it comes to word problems and geometry. Regarding word problems, females with LDs in mathematics tend to do better than males. Males tend to be more analytical and visual while females are more verbal and relational (Devine et al., 2013). It is essential for educators to be aware of these differences when teaching students with learning disabilities in mathematics and adjust their instructional methods accordingly.
Although math skills are thought to be universal, skills vary significantly from one culture to another. This is particularly true when it comes to numerical concepts and skills. For instance, in Western cultures, math is often taught in a linear fashion, with a heavy emphasis on memorization and rote learning. In contrast, many Asian cultures emphasize understanding mathematical concepts and finding creative solutions to problems (Cvencek et al., 2011). This can make it difficult for students from different cultures to succeed in Western math classes.
Contributing Factors
Neurological
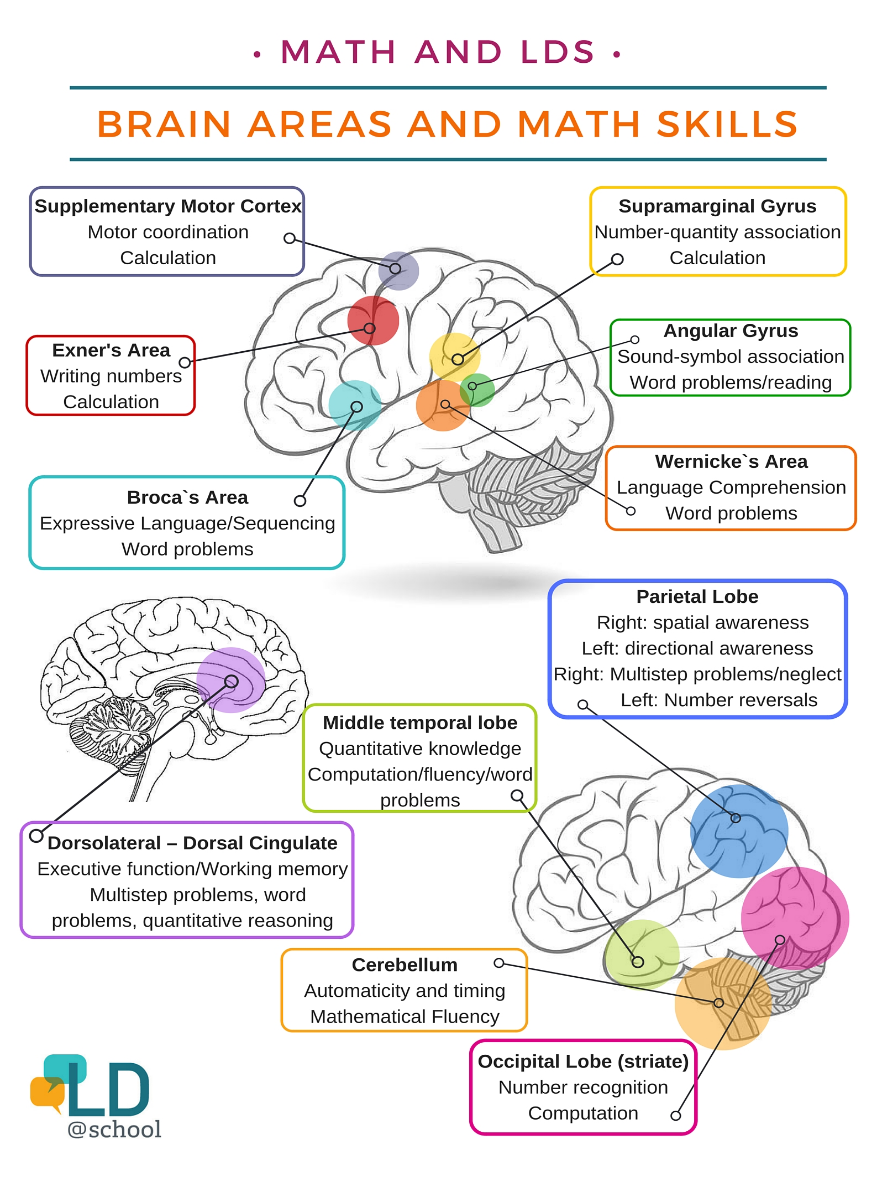
It is now well-accepted that LDs in mathematics have a neurological basis. Numerous imaging studies show children with LDs in mathematics have abnormalities in specific brain regions that are important for mathematical ability. Findings suggest that LDs in mathematics are caused by problems in the way the brain processes numeric and spatial information. As shown in Figure 5, central brain regions involved in mathematical skills development are the parietal lobe, frontal lobe, and cerebellum. The parietal lobe is involved in spatial awareness, directional awareness, multistep problems, and number reversals. Individuals with damage to the parietal lobe often have difficulty with these tasks. The frontal lobe is involved in higher-level mathematical processes (Arsalidou et al., 2018). It includes areas like the supplementary motor cortex responsible for motor coordination and calculation, Exner’s area involved in writing numbers and calculation, and Broca’s area responsible for expressive language and sequencing word problems, which are helpful for problem-solving and reasoning (Kubas & Hale, 2019). Individuals with damage to the frontal lobe often have difficulty with these tasks. The cerebellum is involved in a variety of mathematical processes and fluency. Individuals with damage to the cerebellum often have difficulty with these tasks.
Figure 5
Brain Areas and Math Skills
https://www.ldatschool.ca/evidence-based-interventions-for-math/
Genetic
Individuals with the disorder tend to have genetic markers for attention deficit hyperactivity disorder (ADHD) and other learning disabilities. While the exact cause of LDs in mathematics is unknown, it is believed to be the result of a combination of genetic and environmental factors (Carvalho & Haase, 2019). This theory is supported by identical twins being more likely to have LDs in mathematics than fraternal twins, and that the disorder tends to run in families. In addition, brain imaging studies reveal abnormalities in the structure and function of the brains of individuals with learning disabilities in mathematics, providing further evidence for a neurological basis for the condition. Heritability also plays a significant role in LDs in mathematics. Studies show children with LDs in mathematics are more likely to have relatives with the condition, suggesting a strong genetic component. However, heritability is not the sole contributing factor for LDs in mathematics.
Epigenetic factors may also play a role in the development of LDs in mathematics. Hassan (2021) reveals that individuals with math disabilities are more likely to show changes in the expression of genes involved in neurotransmission, cell proliferation, and synapse formation. These changes suggest that epigenetic factors may contribute to the development of LD in mathematics by affecting the way the brain processes information.
Symptoms and Diagnostic Criteria
Similar to the criteria for learning disabilities in reading, according to the DSM-V (2013), individuals are diagnosed with significant impairment in mathematical ability if persistent difficulties occur for at least six months regardless of resources and support to help with number facts, number sense, calculation, and reasoning. Children diagnosed with learning disabilities in mathematics display lower mathematical ability compared to individuals of the same chronological age. Children at risk for developing LDs in mathematics have difficulty learning and recalling basic number facts, understanding math language (e.g., terms used in formulas), understanding mathematics operations (i.e., addition, subtraction, multiplication, and division), and planning and solving mathematics problems. Children may use fingers to count instead of using more advanced strategies like mental math, and they tend to avoid situations that require an understanding of numbers or calculations (The Dyslexia Association, 2018).
Assessment Process
The assessment process for learning disabilities in mathematics typically involves administering a standardized achievement test. The WIAT-III can be used to assess LDs in mathematics. Another test is the Group Mathematics Assessment and Diagnostic Evaluation (GMADE), which assesses areas in math that students need help with. Another tool is KeyMath-3 Diagnostic Assessment (KeyMath-3 DA), which evaluates mathematical concepts and skills. The Feifer Assessment of Mathematics (FAM) is a scale used to examine the neurodevelopmental processes that underlie children’s ability to attain and proficiently use mathematics knowledge. The scale informs appropriate interventions for children with LDs in mathematics. In general, assessment tools are used to support planning and implementing interventions, and monitoring and evaluating the intervention process.
Supports and Interventions
Similar to learning disabilities in reading, early intervention for LDs in mathematics is paramount. One evidence-based intervention is number sense training. This intervention helps individuals develop a better understanding of number structure. This can be done through activities such as estimating quantities, comparing magnitudes, and using mental arithmetic. Number sense training is effective in improving math skills and may also help to improve working memory and executive functioning (Fletcher et al., 2018).
Other interventions for teachers to support students with difficulties in mathematic facts are the Drill and Practice, which aims to support children to learn and retrieve math facts from their long-term memory storage, and Cover-Copy-Compare. These methods use modelling, guided practice, frequent administration, practice, self-management, reinforcement and feedback to help students store math facts in their long-term memories (Kubas & Hale, 2019). Besides intervention and support, there are some methods that prove ineffective. One of those is using manipulatives to teach math concepts. Although manipulatives can be helpful, they should not be the only method used to teach math (Geary, 2011).
Reading Disability Versus Mathematics Disability
Given that reading disabilities and math disabilities share some common symptoms, it is not surprising that they are often confused with one another. However, there are some critical ways in which they differ. For instance, people with reading disabilities often have difficulty understanding written language, while people with math disabilities often have trouble understanding symbols and numbers (Weitnauer et al., 2016). In addition, people with reading disabilities tend to struggle with phonemic awareness, fluency, and text comprehension, while people with math disabilities tend to struggle with conceptual understanding and procedural knowledge. As a result, it is important to assess patients carefully to accurately diagnose their condition. Only then can appropriate treatment be provided.
Learning Disabilities in Writing
Terminology used for disabilities in writing can vary across contexts. It is essential for readers to understand that, in some cases, various terminology may be used to refer to the same condition(s). Learning disabilities/disorders associated with writing fall under “specific learning disorders” in the DSM-V (American Psychiatric Association, 2013). The more descriptive terminology, “dysgraphia” often appears in clinical and educational resources like LDAC. However, SLD in written expression is not distinctly separate from dysgraphia; these are simply two different ways of referring to the same condition.
Dysgraphia
Dysgraphia is one of the least understood types of specific learning disability/disorder (SLD). Additionally, dysgraphia is one of the few SLDs not characterized by a reading disorder. Regardless, it comes with significant challenges for those who experience it. So, what exactly is dysgraphia? Dysgraphia is as an umbrella term for difficulties with written expression. There are two types of dysgraphia: acquired dysgraphia and developmental dysgraphia. Acquired dysgraphia typically occurs from an injury or neurodegenerative condition (e.g., Alzheimer’s disease) while developmental dysgraphia is apparent during early developmental periods when children begin practicing written expression. Furthermore, developmental dysgraphia may be thought of as a smaller “umbrella” which also contains several (sometimes contested in terms of definition) sub-types (Chung et al., 2020; Forbes et al., 2004). For this online resource concerning school psychology, our focus is on developmental dysgraphia.
Demographics
Canadian dysgraphia statistics are either non-existent or very difficult to find. However, Statistics Canada (2012) published survey data indicating approximately 2.3% of the Canadian population is living with a learning disability. It is stated that conditions such as dysgraphia are included in survey data; however, prevalence rates for distinct types of LDs (e.g., dysgraphia) are unclear (Government of Canada, 2015). Similarly, there are no global statistics for the prevalence of dysgraphia; some researchers suggest this is due to high variability and lack of consistency in definitions (Chung et al., 2020). Like Statistics Canada data, the DSM-V states the global prevalence of SLDs, including writing, is approximately 5%-15% for school-age children, though it does not consider prevalence for different types of SLDs like dysgraphia (American Psychiatric Association, 2013). Some research estimates that the prevalence of dysgraphia in school-aged children ranges from 5% to as high as 27% (Van Hartingsveldt et al., 2011).
Symptoms and Diagnostic Criteria
Subtypes of developmental dysgraphia (i.e., spatial, motor, dyslexic, phonological, lexical) are associated with distinct symptom profiles involving either impairment in writing due to spelling/orthographic coding or impairments in writing itself (due to motor and/or letter spacing difficulties) (McCloskey & Rapp, 2017; Berninger & May, 2011; Van Hoorn et al., 2013). Orthographic coding refers to the storing of written words into working memory while analyzing letters, or the ability to store permanent memories of written words with their meaning and pronunciation (International Dyslexia Association, 2022). Individuals with motor dysgraphia are distinguished by abnormal finger-tapping speed (relative to the other four subtypes). In contrast, individuals with spatial dysgraphia have difficulties with letter spacing. “Dyslexic dysgraphia” gets its name from spelling difficulties typically experienced by people with this subtype but, unlike dyslexia, it is not a reading disability. Spelling difficulties are seen with lexical dysgraphia; however, writing ability for commonly used words is preserved. Similarly, phonological dysgraphia involves spelling difficulty associated with impaired phoneme memorization and improper phoneme blending (Deuel, 1995).
Figure 6
Five Hypothesized Subtypes of Dysgraphia
|
Dyslexic Dysgraphia |
Motor Dysgraphia |
Spatial Dysgraphia |
Phonological Dysgraphia |
Lexical Dysgraphia |
|
Spelling errors |
Impaired fine motor skills and dexterity |
Impaired visual-spatial skills |
Impaired ability to memorize phonemes |
Difficulty with spelling unfamiliar words |
|
Difficulty with writing |
Difficulty with writing |
Difficulty with letter spacing |
Difficulty spelling phonetically irregular or unfamiliar words |
Reliance on sounding out unfamiliar word letters when writing
|
|
Preserved drawing ability |
Difficulties with drawing |
Difficulties with drawing |
Preserved drawing ability |
Preserved ability for spelling commonly used words |
|
Preserved ability to copy written text |
Preserved ability to spell orally |
Preserved ability to spell orally |
Inappropriate blending of phonemes
|
Preserved writing ability |
|
Typical finger-tapping speed |
Abnormal finger-tapping speed |
Typical finger-tapping speed |
Typical finger-tapping speed |
Typical finger-tapping speed |
Note: Made using Microsoft Word. (Deuel, 1995; Chung et al., 2020).
The Learning Disabilities Association of Canada (LDAC) provides a more precise definition of dysgraphia, noting it involves numerous brain regions associated with vocabulary, grammar, hand-movement, and memory that affect writing abilities. Dysgraphia can include difficulties with spelling and writing thoughts down (Learning Disabilities Association of Canada, 2018). Information specific to dysgraphia, as discussed by LDAC, may assist professionals in educational and clinical settings and provide psychoeducational resources. Although specific diagnostic criteria for the term “dysgraphia” is not offered in the DSM-V (Educational Psychologist, 2016), the American Psychiatric Association recognizes dysgraphia on its website as a specific learning disorder characterized by difficulties writing thoughts onto paper (American Psychiatric Association, 2021). Both the LDAC and DSM-V are valuable resources when understanding SLDs like dysgraphia and can be thought of as complementary tools.
Understood. (2019). What is dysgraphia in kids? [Video].
https://www.youtube.com/watch?v=_JYphwPhNp8
Contributing Factors
Neurological
Divergence of neurological functioning plays a vital role in all learning disabilities/ disorders, including dysgraphia. The classification of dysgraphia subtypes, neurological correlates, and symptomology is an active area of research and scientific discussion (Chung et al., 2020). Interestingly, there are similarities and key differences in neurological regions associated with spelling compared to handwriting. Based on previous, but limited, research, there are areas of overlap in several areas in the frontal lobe, temporal and parietal lobes, and the cerebellum (Richards et al., 2009)—all regions associated with visuospatial and verbal-analytic reasoning (Chen et al., 2017).
Richards and colleagues (2009) found fMRI activity in four brain regions associated with writing, while activity in sixteen regions was associated with spelling. Research on individuals with acquired dysgraphia (i.e., resulting from stroke lesions) demonstrates a correlation between orthographic long-term memory impairment and altered structure in the left-posterior frontal lobe and left-ventral temporal cortex. There was also a relationship between orthographic working memory impairment and altered structure in the left parietal cortex (Rapp et al., 2016). In a review of the scientific literature, Van Hoorn and colleagues (2013) conclude that the cerebellum and cortical areas for all lobes of the brain are consistently involved in pediatric dysgraphia. However, the extent to which specific neurological regions are involved varies based on symptoms and severity. For some children altered neurological functioning is associated only with the cerebellum or specific areas of the cortex, while for others altered functioning is associated with more globally widespread neurological networks (Van Hoorn et al., 2013).
Figure 7
Human Brain Anatomy.
https://pixabay.com/vectors/brain-human-anatomy-organ-medicine-148131/
Epigenetic
Epigenetics considers the complex relationships between biological, genetic, behavioural, and socioenvironmental factors. Epigenetic changes can either switch “on” or “off” certain gene expressions via a process known as methylation. Epigenetic changes alter how DNA expression is “read” by the body, rather than altering the DNA sequence itself (U.S. Department of Human & Health Services, 2022). Under specific learning disorders, the DSM-V briefly acknowledges interactions of epigenetic, genetic, and environmental factors that contribute to biological observations of SLD (American Psychiatric Association, 2013). A study on children with SLDs (which included dysgraphia) suggests that, although epigenetic biomarkers could help identify SLDs at early stages, in practice, it is difficult to pinpoint specific biomarkers given the enormous amount of variability in symptomology, the variability across developmental stages, and lack of clear diagnostic criteria. The authors conclude that more research is needed in this area, as biomarker specification can potentially allow for early intervention (Abbott et al., 2017).
Supports and Interventions
In the case of developmental dysgraphia, more research and interdisciplinary collaboration are key components to better understand the neurophysiological differences associated with symptomology and various subtypes. Previous research indicates that children require more widespread neurological activity for writing tasks than adults (De Guio et al., 2012; Van Hoorn et al., 2013), supporting the notion that developmental period may be critical when conducting research and building interventions. Psychological test batteries can serve as complementary tools to psychiatric assessments to gain insight into specific symptoms and provide supports tailored to individuals diagnosed with developmental dysgraphia. More specifically, several test batteries have been proposed for assessing symptoms of dysgraphia, including the John Hopkins Dysgraphia Battery (JHDB), but do not appear to differentiate between developmental dysgraphia and acquired dysgraphia (aka agraphia) (Balasubramanian, 2005; Gubbay et al., 1995). Other supports that help children with certain types of dysgraphia are writing practice, assistive writing devices, and computer–assisted technology for written tasks in the classroom (Van Hoorn et al., 2013).
Non-Verbal Learning Disabilities
Another category of learning disabilities that is less well known is non-verbal learning disabilities/disorders (NVLD). In the case of NVLD, non-verbal does not refer to difficulties in verbal ability. Instead, non-verbal refers to difficulty in areas outside of verbal ability. People with NVLD tend to show strengths in areas of verbal performance (e.g., vocabulary). However, these individuals have difficulty in visual-spatial reasoning, organization, attention, executive functioning, and motor skills (Learning Disabilities Association of Ontario, 2015). Despite challenges with visual learning, children with NVLD may benefit from auditory methods of learning, considering memory for auditory events is often an area where children with NVLD excel (Government of Alberta, 2022).
Demographics
Non-verbal learning disabilities may be underrepresented in statistical data considering the variability and lack of clear consistency in the definition. It is estimated that approximately 4% of children and adolescents in the U.S. and Canada experience NVLDs (Radesky, 2022). Similarly, across North America, children and adolescents ages 6-19, with NVLDs are estimated to range from 3% to 4% (Margolis et al., 2020). NVLD is a newer term and newer area of research, so there are no consistently agreed upon or well-established diagnostic criteria. Further complicating matters, NVLD shares some characteristics with other conditions, such as attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) though they are distinct conditions (Government of Alberta, 2022; Incháustegui, 2019). This demonstrates the need for more research to help establish clear diagnostic measures and better inform statistical prevalence of NVLD as a distinct type of learning disability.
Symptoms and Diagnostic Criteria
The DSM-V does not currently have a category for non-verbal learning disorder/ disability. However, it does briefly mention non-verbal difficulties under the “specific learning disorder” section of the manual (American Psychiatric Association, 2013). The Learning Disabilities Association of Ontario (LDAO, 2015) has a section on NVLD on its website that gives a detailed understanding of NVLD symptomology. In addition to the aforementioned symptoms, the LDAO notes that children with NVLD often have difficulty understanding the “big picture” in situations, learning new travel routes, showing impulse control, engaging in flexible thinking, interpreting metaphorical meaning, and using fine motor skills (e.g., tying shoelaces). Additionally, a significant discrepancy between verbal comprehension and perceptual reasoning is necessary to establish a clinical diagnosis of NVLD.
Neuropsychological tests to identify symptoms of NVLD include the Category Test, Grooved Pegboard Test, and the Tactual Performance Test (Casey et al., 2012). The Grooved Pegboard Test (GPT) is used to assess motor functioning (Tolle et al., 2019); for this reason, the GPT may be a good measure of motor symptoms of NVLD, as well as motor dysgraphia (discussed in the previous section). Scores on the GPT may also be reflective of attentional and executive functioning (Tolle et al., 2019), two cognitive states typically affected by NVLD (Learning Disabilities Association of Ontario, 2015).
Lafayette Instrument. (2021). Purdue Pegboard Test. [Video].
https://www.youtube.com/watch?v=cvQbo0CzScI
Other tools that can be helpful in identifying symptoms of NVLD are clinical interviews with the child, parents, teachers, as well as standardized questionnaires that focus on areas of psychosocial adjustment and adaptive functioning (Casey et al., 2012). Conditions like ADHD and ASD can often share similarities with NVLD in terms of symptomology. For example, all three conditions involve difficulties in areas of attentional, emotional, and executive functioning, understanding pragmatic language use, and social communication (American Psychiatric Association, 2013; Learning Disabilities Association of Ontario, 2015; Mammarella et al., 2022). One symptom domain unique to NVLD is visual-spatial reasoning, where individuals typically have trouble memorizing and cognitively mapping new routes, buildings, etc. (Mammarella, 2022).
Figure 8
Comparison of Some Symptoms of ADHD, ASD, and NVLD
|
Symptom Domains |
ADHD |
ASD |
NVLD |
|
Visual-spatial |
|
|
✓ |
|
Executive functioning |
✓ |
✓ |
✓ |
|
Attentional processing |
✓ |
✓ |
✓ |
|
Pragmatic language |
✓ |
✓ |
✓ |
|
High co-occurrence with anxiety and depression |
✓ |
✓ |
✓ |
Note: Made using Microsoft Word. (American Psychiatric Association, 2013; Mammarella et al., 2022).
Contributing Factors
Neurological
NVLD, also known as NLD, is a neuropsychological condition and subtype of learning disabilities. Children with NVLD have difficulty in socio-emotional areas, such as understanding non-verbal cues (e.g., facial expressions) (Molenaar-Klumper, 2002). These symptoms are similar to social communication symptoms typically seen in individuals with ASD. For example, “deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication” (American Psychiatric Association, 2013). As with many conditions, co-occurrence is possible, but it is important to note that NVLD and ASD are two distinct neuropsychological conditions.
A recent study found lower connectivity levels between the anterior insula, anterior cingulate, and prefrontal cortex regions for children diagnosed with NVLD relative to children without NVLD. These neurological areas play a key role in social processing. Notably, the study found higher connectivity levels between the same brain regions for children with ASD compared to children with NVLD. This evidence supports the notion that NVLD and ASD are distinct conditions, though they share similarities (Margolis et al., 2019). Another recent study considered neurological regions associated with spatial reasoning, finding there was lower connectivity between the left posterior cingulate cortex (PCC) and the right retrosplenial cortex for children diagnosed with NVLD relative to both children with reading disorders and typically developing controls (Banker et al., 2020).
Children with NVLD may be misdiagnosed with ADHD due to the similarities in symptom profiles. Neurological research can help identify differences in neurological structure and functioning across different neuropsychological conditions like NVLD and ADHD. Goldenring Fine and colleagues (2013) conducted MRI research with children ages 8-18 diagnosed with either NVLD, ASD, or ADHD. They found that the splenium (part of the white-matter-rich corpus callosum that connects the two brain hemispheres) was significantly smaller for children with NVLD relative to children with ASD and children with ADHD.
A recent study in children with either NVLD, ASD, or ADHD employed a block design task paradigm to assess visuospatial reasoning. The findings indicated that children with NVLD experienced significant and consistent impairments in processing speed. They also found some children with ADHD experienced visuo-spatial impairments, while others did not, and that children with ASD were comparable to typically developing controls (Cardillo et al., 2020).
Epigenetic
Although the DSM-V does not include NVLD, non-verbal difficulties and epigenetics are briefly mentioned in the following statement: “(For SLD) the biological origin includes an interaction of genetic, epigenetic, and environmental factors, which affect the brain’s ability to perceive or process verbal or non-verbal information efficiently and accurately” (American Psychiatric Association, 2013). Given NVLD has no established diagnostic criteria or consensus, research is non-existent when it comes to NVLD and epigenetics. Other neurodevelopmental disorders with cognitive symptom profiles are linked to disruptions in epigenetic functioning; these conditions include Rett Syndrome (an X-chromosome-linked dominant neurodegenerative disorder), Coffin-Lowry Syndrome (another X-linked disorder), and Prader-Willi Syndrome (which also has similarities to ASD) (Gropman & Batshaw, 2010). Epigenetic factors involved in NVLD is an area of further research once consistent and universal diagnostic measures are constructed. Some researchers have recently stressed the importance of developing valid and reliable clinical criteria to better inform and supplement neurodevelopmental research specific to NVLD (Mammarella, 2022; Casey et al., 2012).
Supports and Interventions
There are few (if any) evidence-based interventions for NVLD (Broitman et al., 2020). Distinguishing between ADHD and NVLD is especially important when it comes to formulating treatment plans. ADHD tends to be responsive to stimulant medication (e.g., methylphenidate). However, this may not be an appropriate treatment to help manage symptoms of NVLD (DuPaul et al., 2012). One way to develop strong support systems and interventions is by collaborating with community stakeholders, especially adults and children with NVLD and other LDs. Lived experience can make a huge difference.
Given that learning disabilities affect children of all cultural backgrounds, the development of new supports and interventions for LDs, including NVLD, must reflect this. Both multiculturalism (i.e., the commitment to recognize, understand, and value cultural diversity, as well as promote equal opportunities) and cultural responsiveness (i.e., purposefully targeted practices that incorporate cultural backgrounds, beliefs, and values) are essential in psychological consultation, assessment, and beyond (Parker et al., 2020). While it is unfortunate that there is currently no official psychiatric diagnostic measure for non-verbal learning disability/disorder, it can be seen as an opportunity to develop new tools and measures that are both scientifically valid and culturally responsive.
Understood. (2017). Thriving with NVLD: living with nonverbal learning disorder (a personal story). [Video].
https://www.youtube.com/watch?v=wV3ITgrR50U
Chapter Summary
We begin the chapter with a general overview of LDs, including historical perspectives and common misconceptions. Different learning disabilities were discussed, including learning disabilities at the word and text-level, learning disabilities in mathematics, dysgraphia, and non-verbal learning disability. Demographics were provided, along with contributing factors, such as the neurological and epigenetic bases that underlie different types of learning disabilities/disorders. Supports and interventions for various LDs were also discussed from historical and current perspectives.
References
Abbott, R. D., Raskind, W. H., Matsushita, M., Price, N. D., Richards, T., & Berninger, V. W. (2017). Patterns of biomarkers for three phenotype profiles of persisting specific learning disabilities during middle childhood and early adolescence: A preliminary study. Biomarkers and Genes, 1(1), 103.
American Psychiatric Association. (2021). What is specific learning disorder? Retrieved December 1, 2022, from https://www.psychiatry.org/patients-families/specific-learning-disorder/what-is-specific-learning-disorder.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
American Psychiatric Association. (2013). Specific Learning Disorder. In Diagnostic and Statistical Manual of Mental Disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.
American Psychiatric Association. (2013). Autism Spectrum Disorder. In Diagnostic and Statistical Manual of Mental Disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.).
American Psychiatric Association. (1968). Diagnostic and statistical manual of mental disorders (2nd ed.).
Arsalidou, M., Pawliw-Levac, M., Sadeghi, M., Pascual-Leone, J. (2018). Brain areas associated with numbers and calculations in children: Meta-analyses of fMRI studies. Developmental Cognitive Neuroscience, 30, 239–250. https://doi.org/10.1016/j.dcn.2017.08.002
Balasubramanian, V. (2005). Dysgraphia in two forms of conduction aphasia. Brain and Cognition, 57(1), 8-15. https://doi.org/10.1016/j.bandc.2004.08.012
Banker, S. M., Ramphal, B., Pagliaccio, D., Thomas, L., Rosen, E., Sigel, A. N., Zeffiro, T., Marsh, R., & Margolis, A. E. (2020). Spatial network connectivity and spatial reasoning ability in children with nonverbal learning disability. Scientific Reports, 10(1), 561. https://doi.org/10.1038/s41598-019-56003-y
Barry, J. (2006). The effect of socio-economic status on academic achievement (doctoral dissertation).
Beckmann, E., & Minnaert, A. (2018). Non-cognitive characteristics of gifted students with learning disabilities: An in-depth systematic review. Frontiers in Psychology, 9. Doi:10.3389/fpsyg.2018.00504
Berninger, W., V. & May, O., M. (2011). Evidence-based diagnosis and treatment for Specific Learning Disabilities involving impairments in written and/or oral language. Journal of Learning Disabilities, 44(2), 167-183. https://doi.org/10.1177/0022219410391189
Broitman, J., Melcher, M., Margolis, A., Davis, J.M. (2020). Specific interventions. NVLD and Developmental Visual-spatial Disorder in Children, pp. 139-158. https://doi.org/10.1007/978-3-030-56108-6_15
Butterworth, B., Varma, S., Laurillard, D. (2011). Dyscalculia: from brain to education. Science, 332(6033), 1049–1053. https://doi.org/10.1126/science.1201536
Cardillo, R., Claudio, V., & Mammarella, C. I. (2020). A comparison of local-global visuospatial processing in autism spectrum disorder, nonverbal learning disability, ADHD and typical development. Research in Developmental Disabilities, 103. https://doi.org/10.1016/j.ridd.2020.103682
Carotenuto, M., Messina, A., Monda, V., Precenzano, F., Iacono, D., Verrotti, A., Piccorossi, A., Gallai, B., Roccella, M., Parisi, L., Maltese, A., Lavano, F., Marotta, R., Lavano, S. M., Lanzara, V., Ferrentino, R. I., Pisano, S., Salerno, M., Valenzano, A., Esposito, M. (2017). Maternal stress and coping strategies in developmental dyslexia: an Italian multicenter study. Frontiers in Psychiatry, 8. https://doi.org/10.3389/fpsyt.2017.00295
Carvalho, M. R., Haase, V. G. (2019). Genetics of dyscalculia: in search of genes. International Handbook of Mathematical Learning Difficulties, 329–343. https://doi.org/10.1007/978-3-319-97148-3_21
Casey, J. E. (2012). A model to guide the conceptualization, assessment, and diagnosis of nonverbal learning disorder. Canadian Journal of School Psychology, 27(1), 35–57. https://doi.org/10.1177/0829573512436966
Chen, Z., De Beuckelaer, A., Wang, X. & Liu, J. (2017). Distinct neural substrates of visuospatial and verbal-analytic reasoning as assessed by Raven’s advanced progressive matrices. Scientific Reports, 7. https://doi.org/10.1038/s41598-017-16437-8
Chung, P. J., Patel, D. R., & Nizami, I. (2020). Disorder of written expression and dysgraphia: definition, diagnosis, and management. Translational Pediatrics, 9(1), 46–54. https://doi.org/10.21037/tp.2019.11.01
Crisci, G., Caviola, S., Cardillo, R., & Mammarella, I. C. (2021). Executive functions in neurodevelopmental disorders: Comorbidity overlaps between attention deficit and hyperactivity disorder and specific learning disorders. Frontiers in Human Neuroscience, 15, 594234. https://doi.org/10.3389/fnhum.2021.594234
Cvencek, D., Meltzoff, A. N., Greenwald, A. G. (2011). Math-gender stereotypes in elementary school children. Child Development, 82(3), 766–779. https://doi.org/10.1111/j.1467-8624.2010.01529.x
De Guio, F., Jacobson, S. W., Molteno, C. D., Jacobson, J. L., & Meintjes, E. M. (2012). Functional magnetic resonance imaging study comparing rhythmic finger tapping in children and adults. Pediatric Neurology, 46(2), 94–100. https://doi.org/10.1016/j.pediatrneurol.2011.11.019
Deuel, R.K. (1995). Developmental dysgraphia and motor skills disorders. Journal
of Child Neurology, (10)1. https://doi.org/10.1177/08830738950100S103
Devine, A., Soltész, F., Nobes, A., Goswami, U., Szűcs, D. (2013). Gender differences in developmental dyscalculia depend on diagnostic criteria. Learning and Instruction, 27, 31–39. https://doi.org/10.1016/j.learninstruc.2013.02.004
DuPaul, J. G., Gormley, J. M., & Laracy, D. S. (2012). Comorbidity of LD and ADHD: implications of DSM-5 for assessment and treatment. Journal of Learning Disabilities, 46(1), 43-51. https://doi.org/10.1177/0022219412464351
Educational Psychologist. (2016). Diagnosis of dysgraphia. Retrieved December 2, 2022, from https://educational-psychologist.co.uk/sen-resources-blog/2016/1/22/cannot-pass-the-knowledge-of-life-and-language-in-the-uk-test-knoll-1
El Wafa, H. E. A., Ghobashy, S. A. E. L., & Hamza, A. M. (2020). A comparative study of executive functions among children with attention deficit and hyperactivity disorder and those with learning disabilities. Middle East Current Psychiatry 27(64). https://doi.org/10.1186/s43045-020-00071-8
Fletcher, J. M., Lyon, G. R., Fuchs, L. S., & Barnes, M. A. (2018). Learning disabilities: From identification to intervention. Guilford Publications.
Forbes, K. E., Shanks, M. F., & Venneri, A. (2004). The evolution of dysgraphia in Alzheimer’s disease. Brain Research Bulletin, 63(1), 19–24. https://doi.org/10.1016/j.brainresbull.2003.11.005
Fuchs, D., Fuchs, L. S., Mathes, P. G., & Martinez, E. A. (2002). Preliminary evidence on the social standing of students with learning disabilities in PALS and No-PALS Classrooms. Learning Disabilities Research and Practice, 17(4), 205–215. doi:10.1111/1540-5826.00046
Fuchs, L. S., Fuchs, D. (2002). Mathematical problem-solving profiles of students with mathematics disabilities with and without comorbid reading disabilities. Journal of Learning Disabilities, 35(6), 564–574. https://doi.org/10.1177/00222194020350060701
Gayan, J., & Olson, R. K. (2001). Genetic and environmental influences on orthographic and phonological skills in children with reading disabilities. Developmental Neuropsychology, 20(2), 483–507. https://doi.org/10.1207/s15326942dn2002_3
Geary, D. C. (2011). Consequences, characteristics, and causes of mathematical learning disabilities and persistent low achievement in mathematics. Journal of Developmental & Behavioral Pediatrics, 32(3), 250-263.
Gilger, J. W., Pennington, B. F., & Defries, J. C. (1991). Risk for reading disability as a function of parental history in three family studies. Reading and Writing, 3(3-4), 205–217. https://doi.org/10.1007/bf00354958
Goldenring Fine, J., Musielak, A. K., & Semrud-Clikeman, M. (2013). Smaller splenium in children with nonverbal learning disability compared to controls, high-functioning autism and ADHD. Child Neuropsychology, 20(6), 641-661. https://doi.org/10.1080/09297049.2013.854763
Government of Canada. (2015). Learning disabilities among canadians aged 15 years and older. Statistics Canada. Retrieved November 17, 2022, from https://www150.statcan.gc.ca/n1/pub/89-654-x/89-654-x2014003-eng.htm#n01-refa
Government of Alberta. (2022). Non-verbal learning disorder. My Health Alberta. Retrieved November 17, 2022, from https://myhealth.alberta.ca/Health/Pages/conditions.aspx?hwid=te7868
Gregoire, J., & Desoete, A. (2009). Mathematical disabilities—An underestimated topic?. Journal of Psychoeducational Assessment, 27(3), 171-174.
Grigorenko, E. L., Compton, D. L., Fuchs, L. S., Wagner, R. K., Willcutt, E. G., & Fletcher, J. M. (2020). Understanding, educating, and supporting children with specific learning disabilities: 50 years of science and practice. American Psychologist, 75(1), 37–51. http://dx.doi.org/10.1037/amp0000452
Gropman, L. A. & Batshaw, L. M. (2010). Epigenetics, copy number variation, and other molecular mechanisms underlying neurodevelopmental disabilities: new insights and diagnostic approaches. Journal of Developmental Pediatrics, (31)7, 582-591. https://doi.org/10.1097/DBP.0b013e3181ee384e
Gubbay, S., S. & Hubert de Klerk, N. (1995). A study and review of developmental dysgraphia in relation to acquired dysgraphia. Brain & Development, 17, 1-8. https://doi.org/10.1016/0387-7604(94)00110-J
Haft, S. L., Myers, C. A., & Hoeft, F. (2016). Socio-emotional and cognitive resilience in children with reading disabilities. Current Opinion in Behavioral Sciences, 10, 133–141. https://doi.org/10.1016/j.cobeha.2016.06.005
Hassan, T. (2021). Neurotransmitters for math brain: a new finding. Gomal Journal of Medical Sciences, 19(4), 125-126.
Helton, J. J., Gochez-Kerr, T., & Gruber, E. (2018). Sexual abuse of children with learning disabilities. Child Maltreatment, 23(2), 157–165. https://doi.org/10.1177/1077559517733814
Hulme, C., Snowling, M. J. (2016). Reading disorders and dyslexia. Current Opinion in Pediatrics, 28(6), 731–735. https://doi.org/10.1097/mop.0000000000000411
Incháustegui, V., M. (2019). Nonverbal learning disabilities – clinical description about neurodevelopmental disabilities. Archives in Neurology & Neuroscience, 4(1). https://doi.org/10.33552/ANN.2019.04.000579
International Dyslexia Association. (2022). Understanding dysgraphia. Retrieved December 2, 2022, from https://dyslexiaida.org/understanding-dysgraphia/
International Dyslexia Association. (2020). Working memory: the engine for learning. Retrieved December 8, 2022, from https://dyslexiaida.org/working-memory-the-engine-for-learning/
International Dyslexia Association. (2020). Dyslexia and the brain. Retrieved December 6, 2022, from https://dyslexiaida.org/dyslexia-and-the-brain/
Jagger-Rickels, A. C., Kibby, M. Y., Constance, J. M. (2018). Global gray matter morphometry differences between children with reading disability, ADHD, and comorbid reading disability/ADHD. Brain and Language, 185, 54–66. https://doi.org/10.1016/j.bandl.2018.08.004
Jordan, J. A., Wylie, J., & Mulhern, G. (2010). Phonological awareness and mathematical difficulty: a longitudinal perspective. The British Journal of Developmental Psychology, 28(Pt 1), 89–107. https://doi.org/10.1348/026151010×485197
Kubas, H. A., & Hale, J. B. (2019). LDS in mathematics: evidence-based interventions, strategies, and resources. LD at School. Retrieved December 7, 2022, from https://www.ldatschool.ca/evidence-based-interventions-for-math/
Learning Disabilities Association of Canada. (2021). LD basics. https://www.ldac-acta.ca/learn-more/ld-basics/
Learning Disabilities Association of Canada. (2018). Common LD terms. Retrieved November 17, 2022, from https://www.ldac-acta.ca/common-ld-terms/
Learning Disabilities Association of Ontario. (2015). Nonverbal learning disability. Retrieved November 17, 2022, from https://www.ldao.ca/introduction-to-ldsadhd/articles/about-lds/nonverbal-learning-disability/
LeFevre, J. A., Fast, L., Skwarchuk, S. L., Smith‐Chant, B. L., Bisanz, J., Kamawar, D., & Penner‐Wilger, M. (2010). Pathways to mathematics: Longitudinal predictors of performance. Child development, 81(6), 1753-1767.
Malcolm, U. (2022). Evidence-based assessment in the science of reading. LD School. Retrieved December 8, 2022, from https://www.ldatschool.ca/evidence-based-assessment-reading/
Malekpour, M., & Aghababaei, S. (2013). The effect of executive functions training on the rate of executive functions and academic performance of students with learning disability. International Journal of Developmental Disabilities, 59(3), 145–155. DOI: 10.1179/2047387712y.000000000
Mammarella, I. C. (2022). Time to recognize nonverbal learning disability to foster advances in Its research. Journal of the American Academy of Child and Adolescent Psychiatry, 61(2), 120–121. https://doi.org/10.1016/j.jaac.2021.05.015
Mammarella, I. C., Cardillo, R., & Semrud-Clikeman, M. (2022). Do comorbid symptoms discriminate between autism spectrum disorder, ADHD and nonverbal learning disability? Research in Developmental Disabilities, 126. https://doi.org/10.1016/j.ridd.2022.104242
Margolis, A. E., Broitman, J., Davis, J. M., Alexander, L., Hamilton, A., Liao, Z., Banker, S., Thomas, L., Ramphal, B., Salum, G. A., Merikangas, K., Goldsmith, J., Paus, T., Keyes, K., & Milham, M. P. (2020). Estimated prevalence of nonverbal learning disability among North American children and adolescents. JAMA Network Open, 3(4). https://doi.org/10.1001/jamanetworkopen.2020.2551
Margolis, A. E., Pagliaccio, D., Thomas, L., Banker, S., & Marsh, R. (2019). Salience network connectivity and social processing in children with nonverbal learning disability or autism spectrum disorder. Neuropsychology, 33(1), 135–143. https://doi.org/10.1037/neu0000494
Mayo Foundation for Medical Education and Research. (2022). Dyslexia. Mayo Clinic. Retrieved November 16, 2022, from https://www.mayoclinic.org/diseases-conditions/dyslexia/symptoms-causes/syc-20353552
McCloskey, M., & Rapp, B. (2017). Developmental dysgraphia: an overview and framework for research. Cognitive Neuropsychology, 34(3-4), 65–82. https://doi.org/10.1080/02643294.2017.1369016
Mitchell, D. (2006). Review of whitnesses to change: families, learning difficulties and history. British Journal of Learning Disabilities, 34(2), 124–125. doi:10.1111/j.1468-3156.2006.00396.x
Molenaar-Klumper, M. (2002). In non-verbal learning disabilities: characteristics, diagnosis, and treatment within an educational setting (pp. 23–37). Jessica Kingsley Publishers. Retrieved from https://books.google.ca/books?hl=en&lr=&id=ZiHv5BdbwtwC&oi=fnd&pg=PA7&ots=bEiWrDta6s&sig=A4B3sQ1D3qbrrTNIxBfChdsBzRI#v=onepage&q&f=false.
National Center for Education Statistics. (2007, M). Peer-assisted learning strategies. U.S. Department of Education. Retrieved December 8, 2022, from https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=WWCirelpa07
Noyes, A., Ritchie, K. C., & King, S. (2022). An exploratory study of pre-service teachers’ evidence-based practice related knowledge, attitudes, and practices. Canadian Journal of School Psychology, 37(4), 385–393.
Parker, J. S., Castillo, J. M., Sabnis, S., Daye, J., & Hanson, P. (2020). Culturally responsive consultation among practicing school psychologists. Journal of Educational and Psychological Consultation, 30(2), 119-155. https://www.tandfonline.com/doi/pdf/10.1080/10474412.2019.1680293?casa_token=nnns5zYPKMAAAAA:T5nlFbyFUFqMMxFy5Fp3G5W2bzBEIrKSOsVszV2rkd34epvXLzGeAhLqcah0iPAMZhrnKdIbXIMl
Pugh, K. R., Mencl, W. E., Jenner, A. R., Katz, L., Frost, S. J., Lee, J. R., Shaywitz, S. E., & Shaywitz, B. A. (2000). Functional neuroimaging studies of reading and reading disability (developmental dyslexia). Mental Retardation and Developmental Disabilities Research Reviews, 6(3), 207–213. https://doi.org/10.1002/1098-2779(2000)6:3<207:aid-mrdd8>3.0.co;2-p
Rapp, B., Purcell, J., Hillis, A. E., Capasso, R., & Miceli, G. (2016). Neural bases of orthographic long-term memory and working memory in dysgraphia. Brain: A Journal of Neurology, 139(2), 588–604. https://doi.org/10.1093/brain/awv348
Radesky, J. (2020). Nonverbal learning disability is more common than previously thought. NEJM Journal Watch. Retrieved November 17, 2022, from https://www.jwatch.org/na51377/2020/04/14/nonverbal-learning-disability-more-common-previously
Richards, T. L., Berninger, V. W., Stock, P., Altemeier, L., Trivedi, P., & Maravilla, K. (2009). Functional magnetic resonance imaging sequential-finger movement activation differentiating good and poor writers. Journal of Clinical and Experimental Neuropsychology, 31(8), 967–983. https://doi.org/10.1080/13803390902780201
Scarborough HS (1990): Very early language deficits in dyslexic children. Child Dev 61: 1728 –1743.
Shaywitz, B. A., Lyon, G. R., & Shaywitz, S. E. (2006). The role of functional magnetic resonance imaging in understanding reading and dyslexia. Developmental Neuropsychology, 30(1), 613–632. https://doi.org/10.1207/s15326942dn3001_5.
SickKids. (2022). Empower™ reading and learning group. Retrieved December 8, 2022, from https://www.sickkids.ca/en/learning/empower-reading/
Slot, E. M., Van Viersen, S., De Bree, E. H., & Kroesbergen, E. H. (2016). Shared and unique risk factors underlying mathematical disability and reading and spelling disability. Frontiers in psychology, 7, 803.
Stecker, P. M., Hodge, J., Griffith, C. A. (2020). Response to intervention framework: An application to school settings. The Clinical Guide to Assessment and Treatment of Childhood Learning and Attention Problems, 77–97. https://doi.org/10.1016/b978-0-12-815755-8.00004-6
Stegemann, K. C. (2016). Learning disabilities in Canada. Learning Disabilities: A Contemporary Journal, 14(1), 53-62.
Ten Braak, D., Lenes, R., Purpura, D. J., Schmitt, S. A., & Størksen, I. (2022). Why do early mathematics skills predict later mathematics and reading achievement? The role of executive function. Journal of Experimental Child Psychology, 214, 105306.
The Dyslexia Association. (2018). The signs of dyscalculia. Retrieved December 3, 2022, from https://www.dyslexia.uk.net/specific-learning-difficulties/dyscalculia/the-signs-of-dyscalculia/
Theodoridou, D., Christodoulides, P., Zakopoulou, V., & Syrrou, M. (2021). Developmental dyslexia: Environment matters. Brain Sciences, 11(6), 782. https://doi.org/10.3390/brainsci11060782
Thornberry, C., & Olson, K. (2005). The abuse of individuals with developmental disabilities. Developmental Disabilities Bulletin, 33(1-2), 1-19. https://files.eric.ed.gov/fulltext/EJ844468.pdf
Tolle, K. A., Rahman-Filipiak, A. M., Hale, A. C., Kitchen Andren, K. A., & Spencer, R. J. (2020). Grooved pegboard test as a measure of executive functioning. Applied Neuropsychology, 27(5), 414–420. https://doi.org/10.1080/23279095.2018.1559165
U.S. Department of Human & Health Services. (2022). What is epigenetics? Centers for Disease Control and Prevention. Retrieved November 17, 2022, from https://www.cdc.gov/genomics/disease/epigenetics.htm
Van Hartingsveldt, M. J., De Groot, I. J., Aarts, P. B., & Nijhuis-Van Der Sanden, M. W. (2011). Standardized tests of handwriting readiness: a systematic review of the literature. Developmental Medicine and Child Neurology, 53(6), 506–515. https://doi.org/10.1111/j.1469-8749.2010.03895.x
Van Hoorn, J.F., Maathuis, C.G.B. and Hadders-Algra, M. (2013). Neural correlates of paediatric dysgraphia. Dev Med Child Neurol, 55, 65-68. https://doi.org/10.1111/dmcn.12310
Vellutino, F. R., Fletcher, J. M., Snowling, M. J., & Scanlon, D. M. (2004). Specific reading disability (dyslexia): What have we learned in the past four decades? Journal of Child Psychology and Psychiatry, 45(1), 2–40. https://doi.org/10.1046/j.0021-9630.2003.00305.x
Weitnauer, E., Landy, D., & Ottmar, E. (2016, December). Graspable math: Towards dynamic algebra notations that support learners better than paper. In 2016 Future Technologies Conference (FTC) (pp. 406-414). IEEE.
Wilson, K. M., & Swanson, H. L. (2001). Are mathematics disabilities due to a domain-general or a domain-specific working memory deficit?. Journal of Learning disabilities, 34(3), 237-248.
